













Thyroid Cancer - Introduction
ON THIS PAGE: You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Thyroid Cancer. Use the menu to see other pages. Think of that menu as a roadmap to this complete guide.
About the thyroid
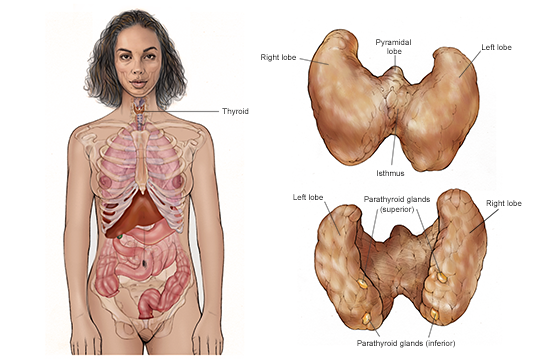
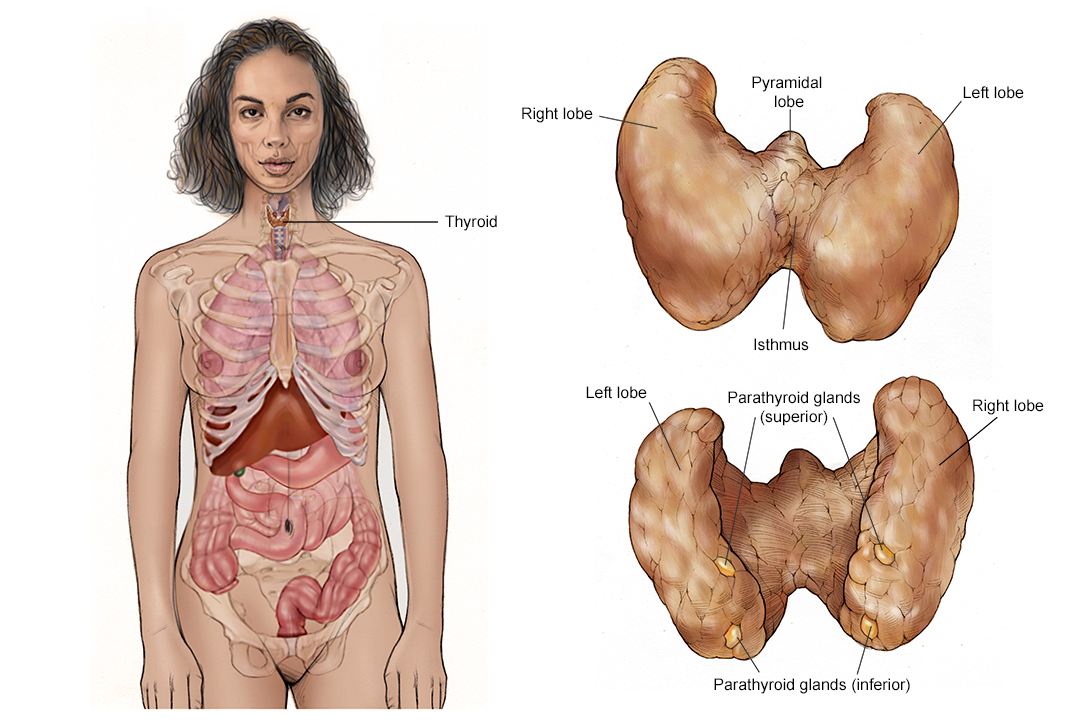
Thyroid cancer begins in the thyroid gland. This gland is part of the endocrine system, which regulates hormones in the body. The thyroid gland absorbs iodine from the bloodstream to produce thyroid hormones to regulate the body's metabolism.
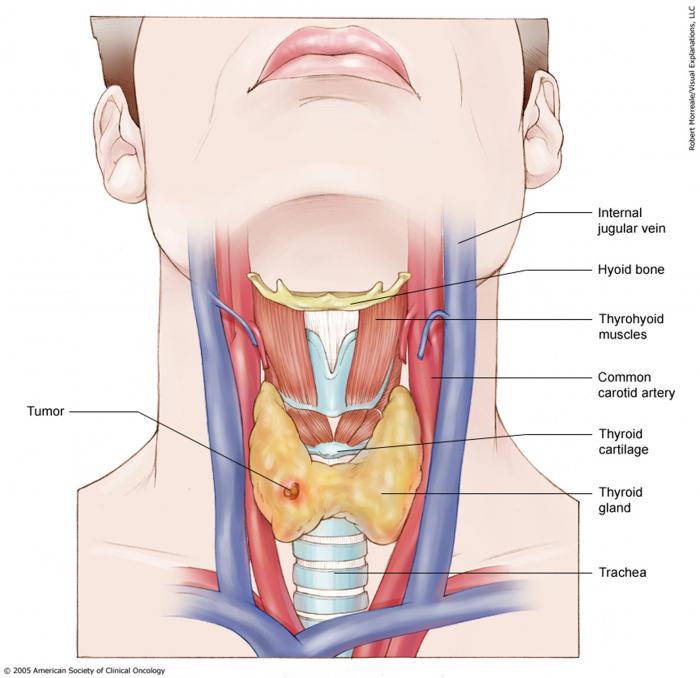
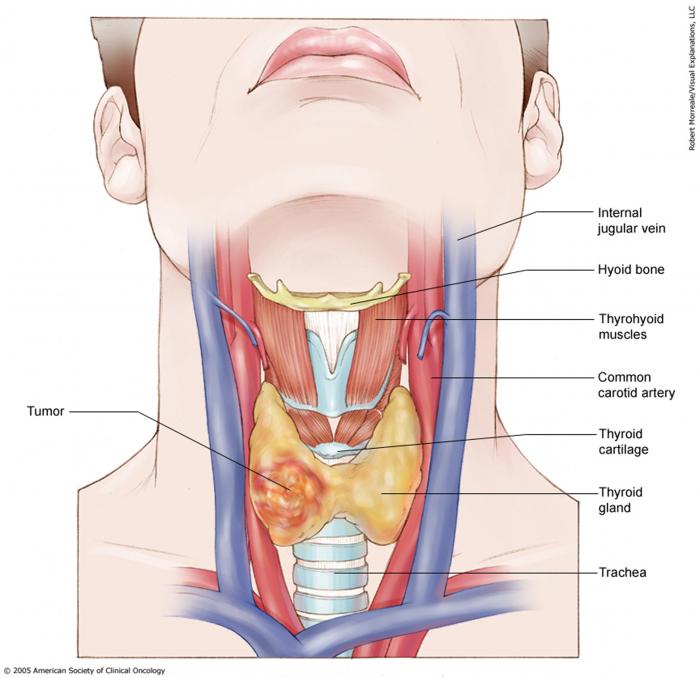
The thyroid gland is located in the front of the neck, just below the larynx (voice box). A normal thyroid gland has 2 lobes, 1 on each side of the windpipe. The lobes are joined by a narrow strip of tissue called the isthmus.
A healthy thyroid gland is barely palpable, which means it is hard to find by touch. A swollen or enlarged thyroid is called a goiter. Most often, a goiter is not caused by cancer. Worldwide, goiters are most often caused by a lack of iodine in the diet. In the United States, most people get enough iodine from salt, so the most common cause of goiters is too much or too little thyroid hormone. Sometimes, the cause of a thyroid goiter is cancer. If a tumor develops in the thyroid, it is felt as a lump in the neck.
About thyroid tumors
Thyroid cancer starts when healthy cells in the thyroid change and grow out of control, forming a mass called a tumor. The thyroid gland contains 2 types of cells:
-
Follicular cells are responsible for the production of thyroid hormone. Thyroid hormone controls the basic metabolism of the body. It controls how quickly calories are burned. This can affect weight loss, weight gain, how fast the heart beats, body temperature, how quickly food moves through the digestive tract, how muscles contract, and how quickly dying cells are replaced. Thyroid hormone is an essential hormone for many body functions and the body needs it to survive.
-
C cells are special thyroid cells that make calcitonin, a hormone involved in calcium metabolism.
A tumor can be cancerous or benign. A cancerous tumor is malignant, meaning it can grow and spread to other parts of the body. A benign tumor means the tumor can grow but will not spread. Thyroid tumors can also be called nodules, and about 90% of all thyroid nodules are benign.
Types of thyroid cancer
There are 5 main types of thyroid cancer:
-
Papillary thyroid cancer . Papillary thyroid cancer develops from follicular cells and usually grow slowly. It is the most common type of thyroid cancer. It is usually found in 1 lobe. About 10% to 20% of papillary thyroid cancer appears in both lobes. It is a differentiated thyroid cancer, meaning that the tumor looks similar to normal thyroid tissue under a microscope. Papillary thyroid cancer can often spread to lymph nodes.
-
Follicular thyroid cancer . Follicular thyroid cancer also develops from follicular cells and usually grows slowly. Follicular thyroid cancer is also a differentiated thyroid cancer, but it is far less common than papillary thyroid cancer. Follicular thyroid cancer rarely spreads to lymph nodes.
Follicular thyroid cancer and papillary thyroid cancer are the most common differentiated thyroid cancers. They are very often curable, especially when found early and in people younger than 50. Together, follicular and papillary thyroid cancers make up about 95% of all thyroid cancer.
-
Hurthle cell cancer . Hurthle cell cancer, also called Hurthle cell carcinoma, is cancer that is arises from a certain type of follicular cell. Hurthle cell cancers are much more likely to spread to lymph nodes than other follicular thyroid cancers.
-
Medullary thyroid cancer (MTC) . MTC develops in the C cells and is sometimes the result of a genetic syndrome called multiple endocrine neoplasia type 2 (MEN2) . This tumor has very little, if any, similarity to normal thyroid tissue. MTC can often be controlled if it is diagnosed and treated before it spreads to other parts of the body. MTC accounts for about 3% of all thyroid cancers. About 25% of all MTC is familial. This means that family members of the patient will have a possibility of a similar diagnosis. The RET proto-oncogene test (see Risk Factors ) can confirm if family members also have familial MTC (FMTC).
-
Anaplastic thyroid cancer. This type is rare, accounting for about 1% of thyroid cancer. It is a fast-growing, poorly differentiated thyroid cancer that may start from differentiated thyroid cancer or a benign thyroid tumor. Anaplastic thyroid cancer can be subtyped into giant cell classifications. Because this type of thyroid cancer grows so quickly, it is more difficult to treat successfully.
In addition, other types of cancer may start in or around the thyroid gland. For lymphoma in the thyroid, read Cancer.Net’s Guide to Non-Hodgkin Lymphoma . For more information on sarcoma in the thyroid, read the Cancer.Net Guide to Sarcoma . For information on a tumor in the nearby parathyroid gland, read Cancer.Net’s Guide to Parathyroid Cancer .
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to another section on Cancer.Net:
-
ASCO Answers Fact Sheet: Read a 1-page fact sheet that offers an introduction to thyroid cancer. This free fact sheet is available as a PDF, so it is easy to print.
-
Cancer.Net en español: Read about Thyroid Cancer in Spanish. Infórmase sobre cáncer de tiroides en español.
-
Find a Cancer Doctor. Search for a cancer specialist in your local area using this free database of doctors from the American Society of Clinical Oncology (ASCO).
-
Cancer Terms. Learn what medical phrases and terms used in cancer care and treatment mean.
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with thyroid cancer and general survival rates. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Statistics
ON THIS PAGE: You will find information about the estimated number of people who will be diagnosed with thyroid cancer each year. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with cancer are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this cancer and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for you individually. The original sources for these statistics are provided at the bottom of this page.
How many people are diagnosed with thyroid cancer?
In 2023, an estimated 43,720 adults (12,540 men and 31,180 women) in the United States will be diagnosed with thyroid cancer. Thyroid cancer is the seventh most common cancer in women. Worldwide, an estimated 586,202 people were diagnosed with thyroid cancer in 2020.
Until recently, thyroid cancer was the most quickly increasing cancer diagnosis in the United States. Researchers believe that part of the reason for the increase was that new, highly sensitive diagnostic tests led to increased detection of smaller cancers. But from 2014, the incidence rate has dropped by around 2% annually as newer criteria for diagnosing thyroid cancer is being used. Thyroid cancer is often diagnosed at a younger age, compared to other cancers in adults. White people are 70% more likely to be diagnosed with the disease than Black people, who have the lowest incidence rate of the disease.
It is estimated that 2,120 deaths (970 men and 1,150 women) from this disease will occur in the United States in 2023. The death rate stayed steady from 2011 to 2020. Women are 3 times more likely to have thyroid cancer than men. However, women and men die at similar rates. This suggests that men have a worse prognosis than women when there is a diagnosis of thyroid cancer. Prognosis is the chance of recovery. In 2020, an estimated 43,646 people worldwide died from thyroid cancer.
What is the survival rate for thyroid cancer?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from thyroid cancer. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having cancer may affect life expectancy. Relative survival rate looks at how likely people with thyroid cancer are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this cancer.
Example: Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for people with thyroid cancer are only an estimate. They cannot tell an individual person if cancer will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for thyroid cancer in the United States is 98%.
The survival rates for thyroid cancer vary based on several factors. These include the stage of cancer, a person’s age and general health, and how well the treatment plan works. Another factor that can affect outcomes is the specific type of thyroid cancer. If the cancer is located only in the thyroid, it is called localized thyroid cancer. About two-thirds of cases are diagnosed at this stage. Around 76% of Black people are likely to be diagnosed with local thyroid cancer compared to 68% of White people. The 5-year relative survival rate is almost 100% for localized papillary, follicular, and medullary thyroid cancers. For localized anaplastic thyroid cancer, the 5-year relative survival rate is 39%.
If thyroid cancer has spread to nearby tissues or organs and/or the regional lymph nodes, it is called regional thyroid cancer. The 5-year relative survival rate for regional papillary thyroid cancer is 99%. For regional follicular cancer, the rate is 98%, and for regional medullary cancer, the rate is 92%. For regional anaplastic thyroid cancer, the rate is 11%.
Medullary and anaplastic thyroid cancers, which together make up about 3% of all thyroid cancers, are the most likely to spread and have the lowest survival rates. If there is distant spread to other parts of the body, it is called metastatic disease. The 5-year relative survival rate for metastatic papillary thyroid cancer is 74%. For metastatic follicular thyroid cancer, the rate is 67%. The rate for metastatic medullary thyroid cancer is 43%. For metastatic anaplastic thyroid cancer, the rate is 4%.
Experts measure relative survival rate statistics for thyroid cancer every 5 years. This means the estimate may not reflect the results of advancements in how thyroid cancer is diagnosed or treated from the last 5 years. Talk with your doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's (ACS) publication Cancer Facts & Figures 2023, the ACS website, and the International Agency for Research on Cancer website. (All sources accessed March 2023.)
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by thyroid cancer. Use the menu to choose a different section to read in this guide.
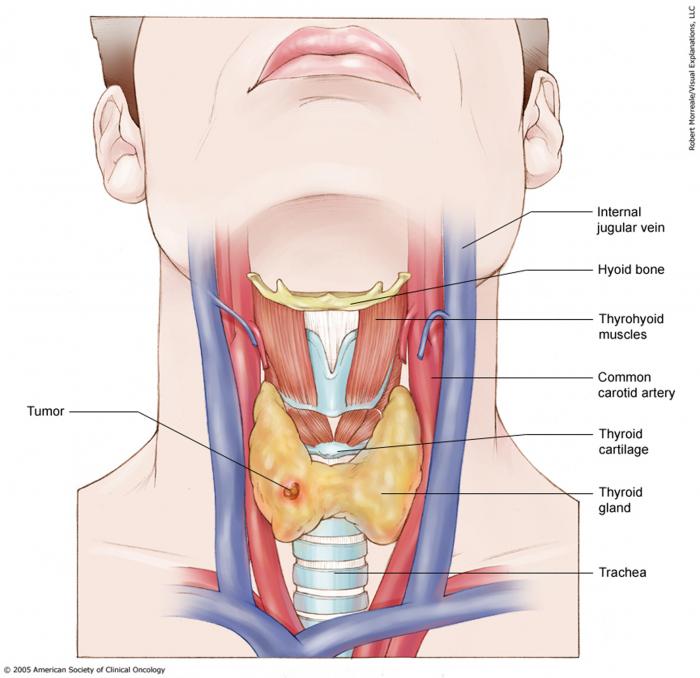
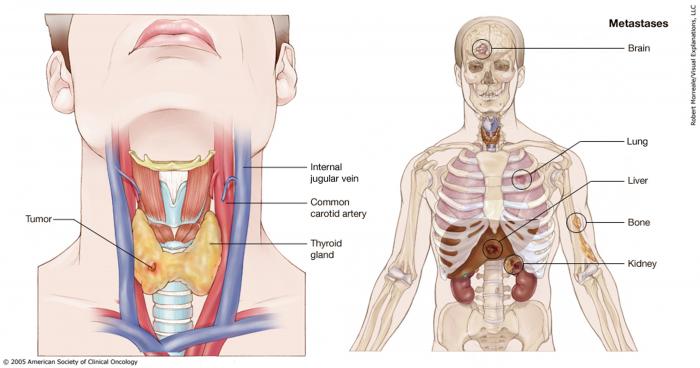
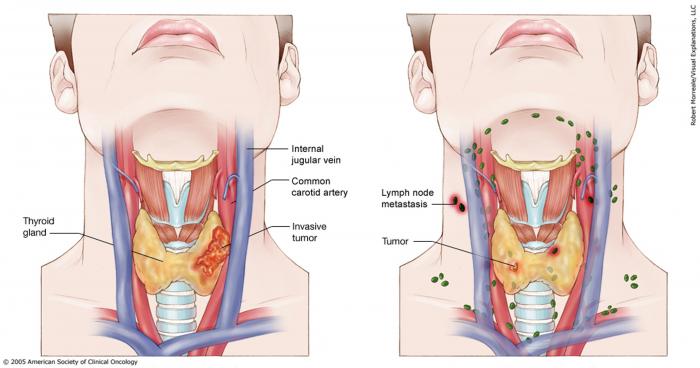
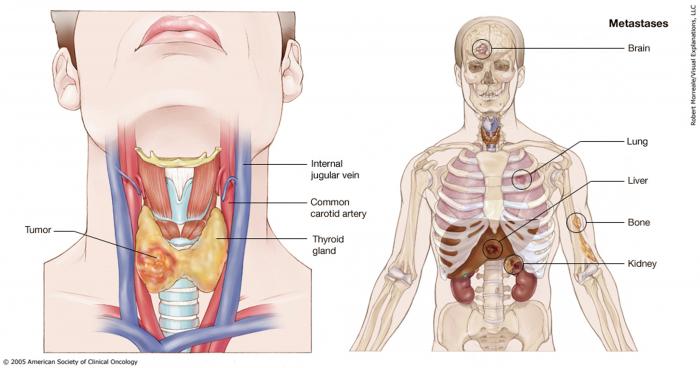
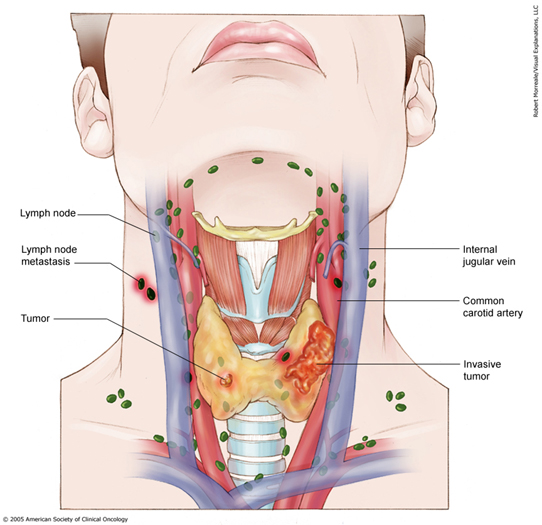
Thyroid Cancer - Medical Illustrations
ON THIS PAGE: You will find a drawing of the main body parts affected by thyroid cancer. Use the menu to see other pages.
The next section in this guide is Risk Factors . It describes the factors that may increase the chance of developing thyroid cancer. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Risk Factors
ON THIS PAGE: You will find out more about the factors that increase the chance of developing thyroid cancer. Use the menu to see other pages.
What are the risk factors for thyroid cancer?
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the development of cancer, most do not directly cause cancer. Some people with several risk factors never develop cancer, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
The following factors may raise a person’s risk of developing thyroid cancer:
Sex. Women are diagnosed with 3 of every 4 thyroid cancers.
Age. Thyroid cancer can occur at any age, but about two-thirds of all cases are found in people between the ages of 20 and 55. Anaplastic thyroid cancer is usually diagnosed after age 60. Older infants (10 months and older) and adolescents can develop medullary thyroid cancer (MTC), especially if they carry the RET proto-oncogene mutation (see below).
Genetics. Some types of thyroid cancer are associated with genetics. Below are some key facts about this disease, genes, and family history. If you are interested in learning more about your personal genetic risk, read this website's article about getting genetic testing .
-
An abnormal RET oncogene, which can be passed from parent to child, may cause MTC. An abnormality may also be called an alteration or mutation. Not everyone with an altered RET oncogene will develop cancer. Blood tests and genetic tests can detect the gene. Once the altered RET oncogene is identified, a doctor may recommend surgery to remove the thyroid gland before cancer develops. People with MTC are encouraged to have genetic testing to determine if a mutation of the RET proto-oncogene is present. If so, genetic testing of parents, siblings, and children will be recommended.
-
A family history of MTC increases a person’s risk.
-
People with MEN2 syndrome are also at risk for developing other types of cancers.
-
A family history of precancerous polyps in the colon, also called the large intestines, increases the risk of developing papillary thyroid cancer.
-
Radiation exposure . Exposure to moderate levels of radiation to the head and neck may increase the risk of papillary and follicular thyroid cancers. Sources of such exposure include:
-
Low-dose to moderate-dose x-ray treatments used before 1950 to treat children with acne, tonsillitis, and other head and neck problems.
-
Radiation therapy for Hodgkin lymphoma or other forms of lymphoma in the head and neck.
-
Exposure to radioactive iodine, also called I-131 or RAI, especially in childhood.
-
Exposure to ionizing radiation, including radioactive fallout from atomic weapons testing during the 1950s and 1960s and nuclear power plant fallout. Examples include the 1986 Chernobyl nuclear power plant accident and the 2011 earthquake that damaged nuclear power plants in Fukushima, Japan. Another source is environmental release of I-131 from atomic weapon production plants.
Diet low in iodine . Iodine is needed for normal thyroid function. In the United States, iodine is added to salt to help prevent thyroid problems.
Race . White people and Asian people are more likely to develop thyroid cancer, but this disease can affect a person of any race or ethnicity.
Breast cancer . A recent study showed that breast cancer survivors may have a higher risk of thyroid cancer, particularly in the first 5 years after diagnosis and for those diagnosed with breast cancer at a younger age. This finding continues to be examined by researchers.
The next section in this guide is Symptoms and Signs . It explains what changes or medical problems thyroid cancer can cause. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Symptoms and Signs
ON THIS PAGE: You will find out more about the changes and medical problems that can be a sign of thyroid cancer. Use the menu to see other pages.
What are the symptoms and signs of thyroid cancer?
It is common for people with thyroid cancer to have few or no symptoms or signs. Symptoms are changes that you can feel in your body. Signs are changes in something measured, like taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem.
Thyroid cancers are often diagnosed by routine examination of the neck during a general physical exam. They are also unintentionally found by x-rays or other imaging scans that were performed for other reasons. People with thyroid cancer may experience one or more of the following symptoms or signs. Sometimes, people with thyroid cancer do not have any of symptoms and signs described below. Or, the cause of a symptom or sign may be a medical condition that is not cancer, such as other thyroid problems or a condition that is not related to the thyroid.
-
A lump in the front of the neck, near the Adam's apple
-
Hoarseness
-
Swollen glands in the neck
-
Difficulty swallowing
-
Difficulty breathing
-
Pain in the throat or neck
-
A cough that persists and is not caused by a cold
If you are concerned about any changes you experience, please talk with your doctor. Your doctor will try to understand what is causing your symptom(s). They may do an exam and order tests to understand the cause of the problem, which is called a diagnosis.
If cancer is diagnosed, relieving symptoms remains an important part of cancer care and treatment. Managing symptoms may also be called "palliative and supportive care," which is not the same as hospice care given at the end of life. This type of care focuses on managing symptoms and supporting people who face serious illnesses, such as cancer. You can receive palliative and supportive care at any time during cancer treatment. Learn more in this guide's section on Coping with Treatment .
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Diagnosis
ON THIS PAGE: You will find a list of common tests, procedures, and scans that doctors use to find the cause of a medical problem. Use the menu to see other pages.
Doctors use many tests to find, or diagnose, cancer. They also do tests to learn if cancer has spread to another part of the body from where it started. If cancer has spread, it is called metastasis. Doctors may also do tests to learn which treatments could work best.
For most types of cancer, a biopsy is the only sure way for the doctor to know if an area of the body has cancer. In a biopsy, the doctor takes a small sample of tissue for testing in a laboratory. If a biopsy is not possible, the doctor may suggest other tests that will help make a diagnosis.
How thyroid cancer is diagnosed
There are different tests used for diagnosing thyroid cancer. Not all tests described here will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
-
The type of cancer suspected
-
Your signs and symptoms
-
Your age and general health
-
The results of earlier medical tests
The following tests may be used to diagnose thyroid cancer:
-
Physical examination . The doctor will feel the neck, thyroid gland, throat, and lymph nodes (the small, bean-shaped organs that help fight infection) in the neck for unusual growths or swelling. If surgery is recommended, the larynx may be examined at the same time with a laryngoscope, which is a thin, flexible tube with a light.
-
Blood tests . There are several types of blood tests that may be done during diagnosis and to monitor the patient during and after treatment. This includes tests called tumor marker tests . Tumor markers are substances found at higher-than-normal levels in the blood, urine, or body tissues of some people with cancer. Blood testing may include:
-
Thyroid hormone levels . As explained in the Introduction , thyroid hormones regulate a person’s metabolism. The doctor will use this test to find out the current levels of the thyroid hormones triiodothyronine (T3) and thyroxine (T4) in the body.
-
Thyroid-stimulating hormone (TSH) . This blood test measures the level of TSH, a hormone produced by the pituitary gland near the brain. If the body is in need of thyroid hormone, the pituitary gland releases TSH to stimulate production.
-
Tg and TgAb . Thyroglobulin (Tg) is a protein made naturally by the thyroid as well as by differentiated thyroid cancer. After cancer treatment, there should be very low levels of thyroglobulin in the blood since the goal of treatment is to remove all thyroid cells. If Tg is rising after surgery and/or radioactive iodine, it may be a sign of more cancer. A tumor marker test may be done to measure the body’s Tg level before, during, and/or after treatment. There is also a test for thyroglobulin antibodies (TgAb), which are proteins produced by the body to attack thyroglobulin that occur in some patients. If TgAb is found, it is known to interfere with the results of the Tg level test.
-
Medullary type-specific tests . If medullary thyroid cancer (MTC) is a possibility, the doctor will order tumor marker tests to check for high calcitonin and carcinoembryonic antigen (CEA) levels. The doctor should also recommend a blood test to look for the presence of RET proto-oncogenes (see Risk Factors ), particularly if there is a family history of MTC.
-
-
Ultrasound . An ultrasound creates a picture of the internal organs using sound waves. An ultrasound wand or probe is guided over the skin of the neck area. High-frequency sound waves create a pattern of echoes that show the doctor the size of the thyroid gland and specific information about any nodules, including whether a nodule is solid or a fluid-filled sac called a cyst.
-
Biopsy. The way to determine whether a nodule is cancerous or benign is through a biopsy. A biopsy is the only way to make a definite diagnosis, even if other tests can suggest that cancer is present. During biopsy, the doctor removes cells from the nodule that are then examined by a cytopathologist. A cytopathologist is a doctor who specializes in analyzing cells and tissue to diagnose disease. This test is often done with the help of an ultrasound (see above).
A biopsy for thyroid nodules will be done in 1 of 2 ways:-
Fine needle aspiration . This procedure is usually performed in a doctor’s office or clinic. It is an important diagnostic step to find out if a thyroid nodule is benign or cancerous. A local anesthetic may be injected into the skin to numb the area before the biopsy. The doctor inserts a thin needle into the nodule and removes cells and some fluid. The procedure may be repeated 2 or 3 times to get samples from different areas of the nodule. A report of the results of this test is created by the cytopathologist. The test results can come back as positive, meaning there are cancerous cells, or negative, meaning there are no cancerous cells. The test can also be undetermined, meaning it is not clear whether cancer is there.
-
Surgical biopsy . If the needle aspiration biopsy is not clear, the doctor may suggest a biopsy in which the nodule and possibly the affected lobe of the thyroid will be removed using surgery. Removal of the nodule alone is usually not recommended due to the potential to incompletely remove the potentially cancerous tumor without enough margins, which is an area of tissue around the nodule. This procedure is usually done under general anesthesia. It may also require a hospital stay.
-
-
Molecular testing of the nodule sample . Your doctor may recommend running laboratory tests on a tumor sample to identify specific genes, proteins, and other factors unique to the tumor. Genetic analysis of your thyroid nodule may allow you to understand the risk of the thyroid nodule being cancerous. Other genetic, protein, and molecular analysis of thyroid cancers can help determine your treatment options , including types of treatments called targeted therapy.
-
Radionuclide scanning . This test may also be called a whole-body scan. This scan will either be done using a very small, harmless amount of radioactive iodine I-131 or I-123, called a tracer. It is used most often to learn more about a thyroid nodule. In this test, the patient swallows the tracer, which is absorbed by thyroid cells. This makes the thyroid cells appear on the scan image, allowing the doctor to see differences between those cells and other body structures.
-
X-ray . An x-ray is a way to create a picture of the structures inside of the body, using a small amount of radiation. For instance, a chest x-ray can help doctors determine if the cancer has spread to the lungs.
-
Computed tomography (CT or CAT) scan . A CT scan creates a 3-dimensional picture of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed, cross-sectional view that shows any abnormalities or tumors. A CT scan can be used to measure the tumor’s size. Sometimes, a special dye called a contrast medium is given before the scan to provide better detail on the image. This dye can be injected into a patient’s vein or given as a pill to swallow.
CT scans are often used in people with thyroid cancer to examine parts of the neck that cannot be seen with ultrasound (see above). Also, CT scans of the chest may be needed to look to see if thyroid cancer has spread to that area of the body. CT scans of the abdomen may be used to see if thyroid cancer has spread to the liver or other sites. Patients with the hereditary form (see Risk Factors ) of MTC may be at risk for developing other types of endocrine tumors in the abdomen; these patients may also have a CT scan of the abdomen.
-
Positron emission tomography (PET) or PET-CT scan . A PET scan creates pictures of organs and tissues inside the body. A PET scan is usually combined with a CT scan (see above), called a PET-CT scan . But you may hear your doctor refer to this procedure just as a PET scan. A small amount of a radioactive sugar substance is injected into the patient’s body. This sugar substance is taken up by cells that use the most energy. Because cancer tends to use energy actively, it absorbs more of the radioactive substance. However, the amount of radiation in the substance is too low to be harmful. A scanner then detects this substance to produce images of the inside of the body .
After diagnostic tests are done, your doctor will review the results with you. If the diagnosis is thyroid cancer, these results also help the doctor describe the cancer. This is called staging.
The next section in this guide is Stages . It explains the system doctors use to describe the extent of the thyroid cancer. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Stages
ON THIS PAGE: You will learn about how doctors describe a cancer’s growth or spread. This is called the stage. Use the menu to see other pages.
READ MORE BELOW:
-
What is cancer staging?
-
TNM staging system
-
Stage groups for papillary or follicular thyroid cancer in a person younger than 55
-
Stage groups for papillary or follicular thyroid cancer in a person 55 and older
-
Stage groups for medullary thyroid cancer
-
Stage groups for anaplastic thyroid cancer
What is cancer staging?
Staging is a way of describing where the cancer is located, if or where it has spread, and whether it is affecting other parts of the body.
Doctors use diagnostic tests to find out the cancer’s stage, so staging may not be complete until all of the tests are finished. Knowing the stage helps the doctor recommend the best kind of treatment, and it can help predict a patient's prognosis. There are different stage descriptions for different types of cancer.
This page provides detailed information about the system used to find the stage of thyroid cancer and the stage groups for thyroid cancer, such as stage II or stage IV.
Return to top
TNM staging system
One tool that doctors use to describe the stage is the TNM system. Doctors use the results from diagnostic tests and scans to answer these questions:
-
Tumor (T): How large is the primary tumor? Where is it located?
-
Node (N): Has the tumor spread to the lymph nodes? If so, where and how many?
-
Metastasis (M): Has the cancer spread to other parts of the body? If so, where and how much?
The results are combined to determine the stage of cancer for each person. For thyroid cancer, there are 5 stages: stage 0 (zero) and stages I through IV (1 through 4). The stage provides a common way of describing the cancer, so doctors can work together to plan the best treatments.
In addition to the TNM system, papillary and follicular thyroid cancers are also staged based on the age of the patient.
Staging can be clinical or pathological. Clinical staging is based on the results of tests done before surgery, which may include physical examinations and imaging tests. Pathological staging is based on what is found during surgery, including a biopsy. In general, pathological staging provides the most information to determine a patient’s prognosis.
Here are more details on each part of the TNM system for thyroid cancer:
Tumor (T)
Using the TNM system, the letter “T” plus a letter or number (0 to 4) is used to describe the size and location of the tumor. Tumor size is measured in centimeters (cm).
Stages may also be divided into smaller groups that help describe the tumor in even more detail. When describing “T” in thyroid cancer, doctors may subdivide the general categories by adding the letter “s” to indicate a solitary (single) tumor or “m” to indicate multifocal (more than 1) tumors. Specific tumor stage information is listed below.
TX: The primary tumor cannot be evaluated.
T0 (T zero): There is no evidence of a tumor.
T1: The tumor is 2 centimeters (cm) or smaller and limited to the thyroid.
T1a: The tumor is 1 cm or smaller.
T1b: The tumor is larger than 1 cm but less than 2 cm.
T2: The tumor is larger than 2 cm but smaller than 4 cm and is limited to the thyroid.
T3: The tumor is larger than 4 cm, but the tumor does not extend beyond the thyroid gland.
T4: The tumor is any size and has extended beyond the thyroid.
T4a : The tumor has spread beyond the thyroid to nearby soft tissues, the larynx, trachea, esophagus, or recurrent laryngeal nerve.
T4b : The tumor has spread beyond the regions in T4a (above).
Node (N)
The “N” in the TNM staging system stands for lymph nodes. Careful evaluation of lymph nodes is an important part of staging thyroid cancer. There are many regional lymph nodes located in the head and neck area. Lymph nodes in other parts of the body are called distant lymph nodes.
NX: The regional lymph nodes cannot be evaluated.
N0 (N zero): There is no evidence of cancer in the regional lymph nodes.
N1: Cancer has spread to the lymph nodes.
N1a: Cancer has spread to the lymph nodes around the thyroid (called the central compartment; the pretracheal, paratracheal, and prelaryngeal lymph nodes).
N1b: Cancer has spread beyond the central compartment, including unilateral cervical (lymph nodes on 1 side of the neck), bilateral cervical (lymph nodes on both sides of the neck), contralateral cervical (the opposite side of the tumor), or mediastinal (the chest) lymph nodes.
Metastasis (M)
The “M” in the TNM system describes whether cancer has spread to other parts of the body, called metastasis.
MX: Distant metastasis cannot be evaluated.
M0 (M zero): Cancer has not spread to other parts of the body.
M1: Cancer has spread to other parts of the body.
Return to top
Stage groups for thyroid cancer
Doctors assign the stage of the cancer by combining the T, N, and M classifications (see above) to say what stage the cancer is.
For thyroid cancer, this staging system differs by tumor type. For papillary or follicular thyroid cancer, staging also depends on the age of the patient.
Stage groups for papillary or follicular thyroid cancer in a person younger than 55
Stage I: This stage describes a tumor (any T) with or without spread to lymph nodes (any N) and no distant metastasis (M0).
Stage II: This stage describes a tumor (any T) with any metastasis (M1) regardless of whether it has spread to the lymph nodes (any N).
Return to top
Stage groups for papillary or follicular thyroid cancer in a person 55 and older
Stage I: This stage describes any small tumor (T1) with no spread to lymph nodes (N0) and no metastasis (M0).
Stage II: This stage describes a larger, noninvasive tumor (T2) with no spread to lymph nodes (N0) and no metastasis (M0).
Stage III : This stage describes a tumor larger than 4 cm but still contained in the thyroid (T3) with no spread to lymph nodes (N0) and no metastasis (M0). Or, any localized tumor (T1, T2, or T3) with spread to the central compartment of lymph nodes (N1a) but no distant spread (M0).
Stage IVA : This stage describes a tumor that has spread to nearby structures (T4a), regardless of whether it has spread to the lymph nodes (any N), but it has not spread to distant places (M0). Or, this describes a localized tumor (T1, T2, or T3) with lymph node spread beyond the central compartment (N1b) but no distant spread (M0).
Stage IVB : This stage describes a tumor that has spread beyond nearby structures (T4b), regardless of spread to lymph nodes (any N), but no distant spread (M0).
Stage IVC : This stage describes all tumors (any T, any N) when there is evidence of metastasis (M1).
Return to top
Stage groups for medullary thyroid cancer
Stage I: This stage describes a small tumor (T1) with no spread to lymph nodes (N0) and no distant metastasis (M0).

Stage II : This stage describes a larger localized tumor (T2 or T3) with no spread to lymph nodes (N0) and no metastasis (M0).

Stage III : This stage describes any localized tumor (T1, T2, or T3) that has spread to the central compartment of lymph nodes (N1a) but has not metastasized (M0).
Stage IVA: This stage describes a tumor that has spread to nearby structures (T4a), regardless of whether it has spread to the lymph nodes (any N), but it has not spread to distant places (M0). Or, this describes a localized tumor (T1, T2, or T3) with lymph node spread beyond the central compartment (N1b) but no distant spread (M0).
Stage IVB : This stage describes a tumor that has spread beyond nearby structures (T4b), regardless of spread to lymph nodes (any N), but no distant spread (M0).
Stage IVC : This stage is used when there is evidence of metastasis (any T, any N, M1).

Return to top
Stage groups for anaplastic thyroid cancer
Stage IV: All anaplastic thyroid tumors are classified as stage IV, regardless of tumor size, location, or metastasis.
Stage IVA : This stage describes an anaplastic tumor that has spread to nearby structures (T4a), regardless of whether it has spread to the lymph nodes (any N), but it has not spread to distant places (M0).
Stage IVB : This stage describes an anaplastic tumor that has spread beyond nearby structures (T4b), regardless of spread to lymph nodes (any N), but no distant spread (M0).
Stage IVC : This stage is used when there is evidence of metastasis (any T, any N, M1).
Recurrent : Recurrent cancer is cancer that has come back after treatment. If the cancer does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis .
Return to top
Used with permission of the American College of Surgeons, Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Eighth Edition (2017) , published by Springer International Publishing.
Information about the cancer’s stage will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment . Use the menu to choose another section to continue reading this guide.
Thyroid Cancer - Types of Treatment
ON THIS PAGE: You will learn about the different treatments doctors use for people with thyroid cancer. Use the menu to see other pages.
This section explains the types of treatments, also known as therapies, that are the standard of care for thyroid cancer. “Standard of care” means the best treatments known. Information in this section is based on medical standards of care for thyroid cancer in the United States. Treatment options can vary from one place to another.
When making treatment plan decisions, you are encouraged to discuss with your doctor whether clinical trials offer additional options to consider. A clinical trial is a research study that tests a new approach to treatment. Doctors learn through clinical trials whether a new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option for all stages of cancer. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
How thyroid cancer is treated
In many cases, a team of doctors who specialize in cancer, called oncologists, works together to create a patient’s overall treatment plan that combines different types of treatments. This is called a multidisciplinary team. For thyroid cancer, this team may include a surgeon, medical oncologist, radiation oncologist, radiologist, nuclear medicine physician, and endocrinologist. Cancer care teams include a variety of other health care professionals, such as physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, dietitians, speech therapists, physical therapists, occupational therapists, and others. Learn more about the clinicians who provide cancer care.
Thyroid cancer is commonly treated by one or a combination of treatments. The common types of treatments used for thyroid cancer are listed below, followed by an outline of common cancer treatments given by stage of disease (see Stages ).
Treatment options and recommendations depend on several factors, including the type and stage of thyroid cancer, possible side effects, and the patient's preferences and overall health. Take time to learn about your treatment options and be sure to ask questions about things that are unclear. Talk with your health care team about the goals of each treatment and what you can expect while receiving the treatment. These types of conversations are called “shared decision-making.” Shared decision-making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision-making is important for thyroid cancer because there are different treatment options.
Cancer treatment is often selected based on guidelines that have been recommended by panels of expert physicians. Although most thyroid cancer is curable, there can be different opinions in how to treat thyroid cancer, particularly regarding which combination of treatments to use and the timing of when treatments are done. Patients are encouraged to seek a second opinion before starting treatment because they should be comfortable with the treatment plan they choose and should ask about clinical trials.
Learn more about making treatment decisions .
-
Surgery
-
Hormone treatment
-
Radioactive iodine therapy
-
External-beam radiation therapy
-
Chemotherapy
-
Targeted therapy
-
Chemotherapy or targeted therapy as part of your treatment plan
-
Physical, emotional, and social effects of cancer
-
Treatment options by stage
-
Metastatic thyroid cancer
-
Remission and the chance of recurrence
-
If treatment does not work
Surgery
Surgery is the removal of the tumor and some surrounding healthy tissue during an operation, called a margin. Surgery may also be called a resection. It is the main treatment for most people with thyroid cancer. A surgical oncologist is a doctor who specializes in treating cancer using surgery. Depending on the size of the thyroid nodule, common surgical options include:
-
Lobectomy. This surgery removes the lobe of the thyroid gland with the cancerous nodule.
-
Near-total thyroidectomy. Also called subtotal thyroidectomy, this is surgery to removes most of the thyroid gland. A small amount of thyroid tissue remains.
-
Total thyroidectomy. This surgery removes the entire thyroid gland.
There are different surgical techniques that can be used for a thyroidectomy:
-
Standard thyroidectomy. During a standard thyroidectomy, a surgeon makes a small incision (or cut) near the base or middle of the neck. This gives the surgeon direct access to the patient’s thyroid gland for the operation. At some cancer centers, newer surgical techniques are being offered to reduce or avoid neck scarring.
-
Endoscopic thyroidectomy. During an endoscopic thyroidectomy, the surgeon makes a single small incision. The surgery is similar to a standard thyroidectomy except that a scope and video monitor are used to guide the procedure rather than surgical loupe magnification, which is special eyewear.
-
Robotic thyroidectomy. The surgeon makes an incision elsewhere, such as in an armpit, the hairline of the neck, mouth or the chest, and then uses a robotic tool to perform the thyroidectomy. Robotic thyroidectomy is not a recommended surgery for thyroid cancer.
Not all surgical options are recommended for all patients. Talk with your doctor about the best approach to treat you.
If there is evidence or risk of spread of cancer to the lymph nodes in the neck, the surgeon may also perform a neck dissection. This is surgery to remove the lymph nodes in the neck. Neck dissection is also called lymphadenectomy.
In general, complications of thyroid surgery may include damage to the nearby parathyroid glands, which help regulate blood calcium levels, excessive bleeding, or wound infections. If the nerves to the larynx are damaged during surgery, this may cause temporary or permanent hoarseness or a “breathy” voice.
Without the thyroid gland, the body stops producing thyroid hormone, which is essential to the body’s function. Hormone replacement (see below), usually given by a daily pill, is the best solution. The patient may also have to take vitamin D and calcium supplements if the parathyroid gland's function is reduced after surgery.
If a tumor cannot be removed using surgery, it is called unresectable or inoperable. The doctor will then recommend other treatment options.
Before surgery, talk with your health care team about the possible side effects from the specific surgery you will have and what you can expect during your recovery. Learn more about the basics of cancer surgery .
Return to top
Hormone treatment
Patients who are treated with surgery usually require thyroid hormone therapy. In addition to replacing the hormone that is needed by the body, the thyroid hormone medication may slow down the growth of any remaining differentiated cancer cells.
Thyroid hormone replacement is levothyroxine (Levothroid, Levoxyl, Synthroid, Tirosint, Unithroid, and other brand names.) Levothyroxine typically comes as a pill that should be taken daily, at the same time each day before meals, so that the body receives a consistent supply. Thyroid hormone replacement is usually prescribed by an endocrinologist, which is a doctor specializing in treating problems with hormones, glands, and the endocrine system.
Also, be sure to talk with your doctor about all other medications you take, including
dietary supplements such as iron or calcium
, to avoid interactions with your thyroid hormone replacement. Read more about
tips to take your medication correctly
.
Thyroid pills may have a few side effects. Occasionally, some patients develop a rash or lose some hair during the first months of treatment.
Hyperthyroidism is a condition in which there is too much thyroid hormone. It may cause weight loss, chest pain, rapid heart rate, irregular heartbeat, cramps, diarrhea, a feeling of being hot, sweats, and bone loss or osteoporosis.
Hypothyroidism is a condition in where there is too little thyroid hormone. It may cause fatigue, weight gain, dry skin and hair, and a feeling of being cold.
The required amount, called a dose, of thyroid hormone is different for every patient and tumor type, and it can change as a person ages or when weight changes. The doctor will monitor your thyroid hormone levels through regular blood tests. Talk with your doctor about what signs to watch for that may mean it is time to adjust your dose of thyroid hormone supplement.
Learn more about the basics of hormone therapy .
Return to top
Radioactive iodine therapy
The thyroid absorbs almost all iodine that enters a body. Therefore, a type of radiation therapy called radioactive iodine (also called I-131, radioiodine, or RAI) can find and destroy thyroid cells not removed by surgery and those that have spread beyond the thyroid. Doctors who prescribe radioactive iodine therapy are usually endocrinologists or nuclear medicine specialists.
Radioactive iodine treatment is an option for some people with papillary, follicular, and Hurthle cell thyroid cancer. Radioactive iodine is used to treat people with a differentiated thyroid cancer that have spread to lymph nodes or to distant sites. A small test dose may be given before full treatment to be sure that the tumor cells will absorb the I-131. People with medullary thyroid cancer (MTC) or anaplastic thyroid cancer should not be treated with I-131.
I-131 therapy is given in either liquid or pill form. People who receive I-131 to destroy cancer cells may be hospitalized for 2 to 3 days, depending on several factors, including the dose given. Patients are encouraged to drink fluids to help the I-131 pass quickly through the body. Within a few days, most of the radiation is gone. Talk with your doctor about ways to limit radiation exposure to other people, including children, who may be around you during this treatment and the days following it.
In preparation for I-131 therapy after surgery, patients are usually asked to follow a low-iodine diet for 2 to 3 weeks beforehand. In addition to the low-iodine diet, patients will be asked to either stop taking thyroid hormone replacement pills temporarily or to receive injections of recombinant thyroid-stimulating hormone (Thyrogen) while taking the hormone replacement. If the hormone therapy is stopped during the preparation period, the patient will likely experience the side effects of hypothyroidism (see above, under Hormone Therapy).
It is important to discuss the possible short-term and long-term effects of I-131 therapy with your doctor. On the first day of treatment, patients may experience nausea and vomiting. In certain circumstances, pain and swelling can occur in the areas where the radioactive iodine is collected. Because iodine is concentrated in salivary gland tissue, patients may experience swelling of the salivary glands. This may result in dry mouth, sometimes called xerostomia .
Large or cumulative doses of radioactive iodine may cause infertility, which is the physical inability to have a child, especially in men. Avoiding pregnancy is recommended for at least 1 year after I-131 treatment. There is a risk of secondary cancer with the use of I-131 (see Follow-up Care ). Occasionally, patients may require repeated treatments over time. However, there is a maximum total dose of radioactive iodine allowed over time, and once reached, this may prevent further use of this treatment.
Return to top
External-beam radiation therapy
External-beam radiation is another type of radiation therapy in which high-energy x-rays are given from a machine outside the body to destroy cancer cells. A doctor who specializes in external-beam radiation therapy is called a radiation oncologist. An external-beam radiation therapy regimen (schedule) usually consists of a specific number of treatments given over a set period of time. When used to treat thyroid cancer, radiation therapy is usually given as outpatient therapy, either in a hospital or clinic, 5 days a week for about 5 to 6 weeks.
For thyroid cancer, external-beam radiation therapy is used only in certain circumstances, typically when later-stage thyroid cancer has spread to critical areas of the neck such as the trachea, voice box, or esophagus. Radiation therapy is usually given after surgery, and treatment is concentrated on a specific area, only affecting cancer cells at that site. Radiation therapy is usually not used to manage thyroid cancer in younger patients.
Side effects depend on the treatment dosage and area and may include redness of the skin, odynophagia (painful swallowing), cough, occasional hoarseness, nausea, and fatigue. Most side effects go away soon after treatment is finished.
Learn more about the basics of external-beam radiation therapy .
Return to top
Therapies using medication
The treatment plan my include medications to destroy cancer cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy. Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body.
This treatment is generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication.
When used, medications are often given through an intravenous (IV) tube placed into a vein using a needle or as a pill or capsule that is swallowed (orally). If you are given oral medications to take at home, be sure to ask your health care team how to safely store and handle them.
The types of medications used to treat thyroid cancer include:
-
Chemotherapy
-
Targeted therapy
Each of these types of therapies is discussed below in more detail. A person may receive only 1 type of medication at a time or a combination of medications given at the same time. They can also be given as part of a treatment plan that includes surgery and/or radiation therapy.
The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications. It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases .
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells. A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A patient may receive 1 drug at a time or a combination of different drugs given at the same time.
The side effects of chemotherapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, hair loss, loss of appetite, and diarrhea. These side effects usually go away after treatment is finished. Learn more about the basics of chemotherapy .
Return to top
Targeted therapy
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of cancer cells and limits damage to normal cells. Learn more about the basics of targeted therapy .
Not all tumors have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, research studies continue to find out more about specific molecular targets in the different types of thyroid cancer and new treatments directed at them.
For papillary and follicular thyroid cancers, the U.S. Food and Drug Administration (FDA) has approved several targeted therapies:
Sorafenib (Nexavar) is approved for later-stage or recurrent differentiated thyroid cancer when I-131 therapy (see above) has not worked.
Lenvatinib (Lenvima, E7080) is approved for later-stage differentiated thyroid cancer when surgery, I-131 treatment, or both have not worked.
Larotrectinib (Vitrakvi) is approved for rare cases of papillary and follicular thyroid cancers that have an NTRK gene fusion mutation.
Entrectinib (Rozlytrek) is approved for thyroid tumors with an NTRK gene fusion mutation.
Selpercantinib (Retevmo) and Pralsetinib (Gavreto) are approved for rare cases of advanced metastatic RET fusion-positive thyroid cancer that requires systemic therapy. They can affect the levels of platelets, certain enzymes, and proteins in the body. These levels need to be monitored every 2 weeks during the first 3 months of treatment and then every month after that.
For MTC, the FDA-approved targeted therapy options include:
Vandetanib (Caprelsa, zd6474) is a type of tyrosine kinase inhibitor that is approved to treat MTC when it cannot be removed surgically, if the disease is worsening, or if the MTC has spread to other parts of the body. Additional blood tests may be needed for people who are taking vandetanib because of possible severe side effects. The blood tests will be used to monitor serum potassium, calcium, magnesium, and thyroid-stimulating hormone (TSH) levels (see Diagnosis ) to regularly check the body's reaction to this medication.
Cabozantinib (Cometriq, Cabometyx, XL184) is a type of tyrosine kinase inhibitor that is approved for metastatic MTC. It is also approved to treat differentiated thyroid cancer that has progressed after prior treatment with VEGFR-targeted therapy in people who cannot receive radioactive iodine treatment.
Selpercatinib (see above) is also approved to treat people with advanced or metastatic RET -mutant MTC.
For anaplastic thyroid cancer, there is 1 targeted therapy combination approved by the FDA:
Dabrafenib (Tafinlar) and trametinib (Mekinist) are approved to treat people with anaplastic thyroid cancer with a specific mutation in the BRAF gene. Dabrafenib is a BRAF inhibitor and trametinib is a MEK inhibitor. This combination is now a standard of care for anaplastic thyroid cancer that cannot be removed surgically or has spread to distant areas.
Before any targeted treatment begins, talk with your doctor about possible side effects for each specific medication and how they can be managed. Common side effects of targeted therapies include skin problems, diarrhea, fatigue, blood pressure problems, constipation, nausea, and vomiting.
Return to top
Chemotherapy or targeted therapy as part of your treatment plan
At this time, the use of other systemic chemotherapy and targeted therapy for the treatment of thyroid cancer is determined on an individual basis and is most often given as part of a clinical trial. See the Latest Research section for more information.
Learn more about the basics of preparing for treatment . The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications. Learn more about your prescriptions by using searchable drug databases .
Return to top
Physical, emotional, social, and financial effects of cancer
Thyroid cancer and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative and supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Palliative and supportive care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after a cancer diagnosis. People who receive palliative and supportive care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments such as chemotherapy, surgery, or radiation therapy, to improve symptoms.
Before treatment begins, talk with your doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative and supportive care options. Many patients also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative and supportive care in a separate section of this website.
Return to top
Treatment options by stage
Almost all thyroid cancers are treated with surgery. If the thyroid cancer is only within the tissues of the neck, both in the thyroid gland and in the lymph nodes, surgery will typically be the first treatment. Patients with later-stage disease may be treated with surgery as well, but other treatments may be done first. Clinical trials may be recommended at any stage as a treatment option.
Hormone therapy and radioactive iodine therapy are only given for papillary, follicular, and Hurthle cell thyroid cancers. MTC and anaplastic thyroid cancers are not managed with radioactive iodine thyroid or thyroid hormone therapy.
Stage I: Surgery, hormone therapy, possible radioactive iodine therapy after surgery
Stage II: Surgery, hormone therapy, possible radioactive iodine therapy after surgery
Stage III: Surgery, hormone therapy, possible radioactive iodine therapy or external-beam radiation therapy after surgery
Stage IV: Surgery, hormone therapy, radioactive iodine therapy, external-beam radiation therapy, targeted therapy, and chemotherapy. Radiation therapy may also be used to reduce pain and other problems. See below for more information, for "Metastatic thyroid cancer."
Return to top
Metastatic thyroid cancer
If the cancer has spread beyond the thyroid to other organs, such as the bones or lungs, it is called metastatic or stage IV thyroid cancer. Also, all anaplastic thyroid tumors are classified as stage IV at the time of diagnosis, regardless of tumor size, location, or spread.
If the diagnosis is stage IV thyroid cancer, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan. Clinical trials might also be an option. Learn more about getting a second opinion before starting treatment, so you are comfortable with your chosen treatment plan.
Your treatment plan may include a combination of surgery, hormone therapy, radioactive iodine therapy, external-beam radiation therapy, targeted therapy, and chemotherapy. Clinical trials on new treatment approaches may also be recommended. Palliative and supportive care will also be important to help relieve symptoms and side effects
For most people, a diagnosis of metastatic cancer is very stressful and difficult to bear. You and your family are encouraged to talk about how you feel with doctors, nurses, social workers, or other members of your health care team. It may also be helpful to talk with other patients, such as through a support group or other peer support program.
Return to top
Remission and the chance of recurrence
A remission is when cancer cannot be detected in the body and there are no symptoms. This may also be called having “no evidence of disease” or NED.
A remission may be temporary or permanent. This uncertainty causes many people to worry that the cancer will come back. While many remissions are permanent, it is important to talk with your doctor about the possibility of the cancer returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the cancer does return. Learn more about coping with the fear of recurrence .
If the cancer returns after the original treatment, it is called recurrent cancer. It may come back in the same place (called a local recurrence), nearby (regional recurrence), or in another place (distant recurrence).
If a recurrence happens, a new cycle of testing will begin to learn as much as possible about it. After this testing is done, you and your doctor will talk about the treatment options.
Often the treatment plan will include the treatments described above, such as surgery, radioactive iodine therapy, targeted therapy, external-beam radiation therapy, hormone therapy, and chemotherapy. However, they may be used in a different combination or given at a different pace. Your doctor may suggest clinical trials that are studying new ways to treat recurrent thyroid cancer. Whichever treatment plan you choose, palliative and supportive care will be important for relieving symptoms and side effects.
People with recurrent cancer sometimes experience emotions such as disbelief or fear. You are encouraged to talk with your health care team about these feelings and ask about support services to help you cope. Learn more about dealing with cancer recurrence .
Return to top
If treatment does not work
Recovery from thyroid cancer is not always possible. If the cancer cannot be cured or controlled, the disease may be called advanced or terminal.
This diagnosis is stressful, and for some people, advanced cancer is difficult to discuss. However, it is important to have open and honest conversations with your health care team to express your feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families and is there to help. Making sure a person is physically comfortable, free from pain, and emotionally supported is extremely important.
Planning for your future care and putting your wishes in writing is important, especially at this stage of disease. Then, your health care team and loved ones will know what you want, even if you are unable to make these decisions. Learn more about putting your health care wishes in writing .
People who have advanced cancer and who are expected to live less than 6 months may want to consider hospice care. Hospice care is designed to provide the best possible quality of life for people who are near the end of life.
You and your family are encouraged to talk with your doctor or a member of your palliative care team about hospice care options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment can make staying at home a workable option for many families. Learn more about advanced cancer care planning .
After the death of a loved one, many people need support to help them cope with the loss. Learn more about grief and loss .
Return to top
The next section in this guide is About Clinical Trials . It offers more information about research studies that are focused on finding better ways to care for people with cancer. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - About Clinical Trials
ON THIS PAGE: You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for people with thyroid cancer. To make scientific advances, doctors create research studies involving volunteers, called clinical trials. Every drug that is now approved by the U.S. Food and Drug Administration (FDA) was tested in clinical trials.
Clinical trials are used for all types and stages of thyroid cancer. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment.
People who participate in clinical trials can be some of the first to get a treatment before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. People are encouraged to talk with their health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a long time after treatment. Talk with your doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result.
Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating thyroid cancer. Even if they do not benefit directly from the clinical trial, their participation may benefit future people with thyroid cancer.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about health insurance coverage of clinical trials .
Sometimes people have concerns that, in a clinical trial, they may receive no treatment by being given a placebo or a “sugar pill.” When used, placebos are usually combined with standard treatment in most cancer clinical trials. Study participants will always be told when a placebo is used in a study. Find out more about placebos in cancer clinical trials.
Patient safety and informed consent
To join a clinical trial, people must participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options so that the person understands how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different from the risks of standard treatment.
-
Explain what will be required of each person in order to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.
-
Describe the purposes of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. You will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time for personal or medical reasons. This may include that the new treatment is not working or there are serious side effects.
Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if the they choose to leave the clinical trial before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all types of cancer. For specific topics being studied for thyroid cancer, learn more in the Latest Research section.
Cancer.Net offers more information about cancer clinical trials in other areas of the website, including a complete section on clinical trials .
There are many resources and services to help you search for clinical trials for XYZ cancer, including the following services. Please note that these links will take you to separate, independent websites:
-
ClinicalTrials.gov. This U.S. government database lists publicly and privately supported clinical trials.
-
World Health Organization (WHO) International Clinical Trials Registry Platform. The WHO coordinates health matters within the United Nations. This search portal gathers clinical trial information from many countries’ registries.
Read more about the basics of clinical trials matching services .
In addition, you can find a free video-based educational program about cancer clinical trials, located in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for thyroid cancer. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about thyroid cancer and how to treat it. Use the menu to see other pages.
Doctors are working to learn more about thyroid cancer, ways to prevent it, how to best treat it, and how to provide the best care to people diagnosed with this disease. The following areas of research may include new options for patients through clinical trials. Always talk with your doctor about the best diagnostic and treatment options for you.
-
New treatments. Clinical trials for thyroid cancer include testing new medications, including drugs known as targeted therapy. As explained in Types of Treatment , targeted therapy is a treatment that targets specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. In addition, researchers are looking at new combinations of chemotherapy and other treatments for all stages and types of thyroid cancer.
-
Molecular tumor testing. Investigations are underway to fine-tune diagnosis and predict treatment outcomes based on the molecular biology of the tumor. Molecular biology is the study of the structure and function of cells at the molecular level. For example, genetic testing and the refinement of RET oncogenes (see Risk Factors ) is an ongoing area of active research. Further knowledge in this area will improve how treatment options are chosen and give more precise prognosis.
-
Data collection. There are efforts underway to create volunteer registries of people with a history of thyroid cancer. This can help doctors research this disease in the future. Participants are asked to provide information, tissue samples, or blood and urine sample.
-
Palliative and supportive care. Clinical trials are underway to find better ways of reducing symptoms and side effects of current thyroid cancer treatments to improve comfort and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in thyroid cancer, explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your doctor or search online clinical trial databases now .
-
Visit the Cancer.Net Blog for news, perspectives, and information about this type of cancer.
-
Get updates from Cancer.Net delivered right to your inbox. Subscribe to the Inside Cancer.Net email newsletter.
-
Visit the website of Conquer Cancer, the ASCO Foundation to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance on how to cope with the physical, emotional, social, and financial changes that cancer and its treatment can bring. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Coping with Treatment
ON THIS PAGE: You will learn more about coping with the physical, emotional, social, and financial effects of cancer and its treatment. Use the menu to see other pages.
Every cancer treatment can cause side effects or changes to your body and how you feel. For many reasons, people do not experience the same side effects even when they are given the same treatment for the same type of cancer. This can make it hard to predict how you will feel during treatment.
READ MORE BELOW:
-
Coping with physical side effects
-
Coping with emotional and social effects
-
Coping with the costs of cancer care
-
Coping with barriers to care
-
Talking with your health care team about side effects
-
Caring for a loved one with thyroid cancer
As you prepare to start cancer treatment, it is normal to fear treatment-related side effects . It may help to know that your health care team will work to prevent and relieve side effects. This part of cancer treatment is called palliative and supportive care. It is an important part of your treatment plan, regardless of your age or the stage of disease.
Coping with physical side effects
Common physical side effects from each treatment option for thyroid cancer are described in the Types of Treatment section. Learn more about side effects of cancer and its treatment, along with ways to prevent or control them . Changes to your physical health depend on several factors, including the cancer’s stage, the length and dose of treatment, and your general health.
Talk with your health care team regularly about how you are feeling. It is important to let them know about any new side effects or changes in existing side effects. If they know how you are feeling, they can find ways to relieve or manage your side effects to help you feel more comfortable and potentially keep any side effects from worsening.
You may find it helpful to keep track of your side effects so it is easier to talk about any changes with your health care team. Learn more about why tracking side effects is helpful .
Sometimes, side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment are called late effects . Treating long-term side effects and late effects is an important part of survivorship care. Learn more by reading the Follow-up Care section of this guide or talking with your doctor.
Return to top
Coping with emotional and social effects
You can have emotional and social effects after a cancer diagnosis. This may include dealing with a variety of emotions, such as sadness, anxiety, fear, anger, or managing stress. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about the diagnosis.
Read a blog from a thyroid cancer survivor about how she coped with her diagnosis. You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your needs.
Return to top
Coping with the costs of cancer care
Cancer treatment can be expensive. It may be a source of stress and anxiety for people with cancer and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their cancer treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Return to top
Coping with barriers to care
Some groups of people experience different rates of new cancer cases and experience different outcomes from their cancer diagnosis. These differences are called “cancer disparities.” Disparities are caused in part by real-world barriers to quality medical care and social determinants of health, such as where a person lives and whether they have access to food and health care. Cancer disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , adults older than 65 , and people who live in rural areas or other underserved communities .
If you are having difficulty getting the care you need, talk with a member of your health care team or explore other resources that help support medically underserved people .
Return to top
Talking with your health care team about side effects
Before starting treatment, talk with your doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should I call about side effects?
Be sure to tell your health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are serious. This discussion should include physical, emotional, social, and financial effects of cancer.
Return to top
Caring for a loved one with thyroid cancer
Family members and friends often play an important role in taking care of a person with thyroid cancer. This is called being a caregiver. Caregivers can provide physical, practical, and emotional support to the patient, even if they live far away. Being a caregiver can also be stressful and emotionally challenging. One of the most important tasks for caregivers is caring for themselves .
Caregivers may have a range of responsibilities on a daily or as-needed basis, including:
-
Providing support and encouragement
-
Talking with the health care team
-
Giving medications
-
Helping manage symptoms and side effects
-
Coordinating medical appointments
-
Providing a ride to and from appointments
-
Assisting with meals
-
Helping with household chores
-
Handling insurance and billing issues
A caregiving plan can help caregivers stay organized and help identify opportunities to delegate tasks to others. It may be helpful to ask the health care team how much care will be needed at home and with daily tasks during and after treatment. Use this 1-page fact sheet to help make a caregiving action plan. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Return to top
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of your symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on anxiety and depression , constipation , diarrhea , and rash that provide a tracking sheet to record the timing and severity of the side effect. These free fact sheets are available as a PDF, so they are easy to print out.
The next section in this guide is Follow-up Care . It explains the importance of checkups after cancer treatment is finished. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Follow-Up Care
ON THIS PAGE: You will read about your medical care after cancer treatment is completed and why this follow-up care is important. Use the menu to see other pages.
Care for people diagnosed with thyroid cancer does not end when active treatment has finished. Your health care team will continue to check that the cancer has not come back, manage any side effects, and monitor your overall health. This is called follow-up care and may include:
-
Physical exams and medical tests. Your follow-up care may include regular physical examinations, medical tests, or both. Doctors want to keep track of your recovery in the months and years ahead. People treated for thyroid cancer are typically asked to return to the doctor’s office every 6 months to a year. At a follow-up care visit, the doctor will conduct a physical examination and blood tests to watch the level of thyroid-stimulating hormone (TSH) suppression and to test for thyroglobulin (Tg, see Diagnosis ). If the thyroid gland has been removed, there should be little or no Tg in the blood. An elevated level may indicate the cancer has returned.
Other blood tests may be done depending on the specific type of thyroid cancer treated. Blood tests also help the doctor determine the correct dose of the patient’s thyroid replacement medication (if needed), which may be adjusted over time as the person gets older.
-
Other follow-up tests. Other follow-up tests may include a chest x-ray, an ultrasound of the neck, a full-body scan, or other imaging tests. If the doctor recommends a procedure that uses radioactive iodine (I-131), patients may have to stop taking their thyroid medication for up to 6 weeks or they may be asked to follow a low-iodine diet for up to 2 weeks before having the test.
-
Tests for long-term side effects. Based on the type of treatment received, the doctor will determine what examinations and tests are needed to check for long-term side effects, including the possibility of secondary cancer. This is particularly important for people who have received I-131 treatment, who may be at higher risk of leukemia and urinary bladder cancer.
-
Breast cancer screening. Young women who are treated for papillary or follicular thyroid cancer have a higher risk of developing breast cancer in the future. They should talk with their doctor about appropriate breast cancer screening recommendations.
-
Cancer rehabilitation. Cancer rehabilitation may be recommended, and this could mean any of a wide range of services, such as physical therapy, occupational therapy, career counseling, pain management, nutritional planning, and/or emotional counseling. The goal of rehabilitation is to help people regain control over many aspects of their lives and remain as independent as possible. Learn more about cancer rehabilitation.
Learn more about the importance of follow-up care .
Watching for recurrence
One goal of follow-up care is to check for a recurrence, which means that the cancer has come back. Cancer recurs because small areas of cancer cells may remain undetected in the body. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms. During follow-up care, a doctor familiar with your medical history can give you personalized information about your risk of recurrence. Your doctor will ask specific questions about your health. Some people may have blood tests or imaging tests done as part of regular follow-up care, but testing recommendations depend on several factors, including the type and stage of cancer first diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results may add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects
Most people expect to have side effects when receiving treatment. However, it is often surprising to survivors that some side effects may linger beyond the treatment period. These are called long-term side effects. Other side effects called late effects may develop months or even years after treatment has ended. Long-term and late effects can include both physical and emotional changes.
Talk with your doctor about your risk of developing such side effects based on your diagnosis, your individual treatment plan, and your overall health. If you had a treatment known to cause specific late effects, you may have certain physical examinations, scans, or blood tests to help find and manage them.
Keeping personal health records
You and your doctor should work together to develop a personalized follow-up care plan. Be sure to discuss any concerns you have about your future physical or emotional health. The American Society of Clinical Oncology (ASCO) offers forms to help keep track of the cancer treatment you received and develop a survivorship care plan when treatment is completed.
This is also a good time to talk with your doctor about who will lead your follow-up care. Some survivors continue to see their oncologist or endocrinologist, while others transition back to the care of their primary care doctor or another health care professional. This decision depends on several factors, including the type and stage of cancer, treatments received, side effects, health insurance rules, and your personal preferences.
If a doctor who was not directly involved in your cancer care will lead your follow-up care, be sure to share your cancer treatment summary and survivorship care plan forms with them, and with all future health care providers. Details about your cancer treatment are very valuable to the health care professionals who will care for you throughout your lifetime.
The next section in this guide is Survivorship . It describes how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Survivorship
ON THIS PAGE: You will read about how to with challenges in everyday life after a cancer diagnosis. Use the menu to see other pages.
What is survivorship?
The word “survivorship” is complicated because it means different things to different people. Common definitions include:
-
Having no signs of cancer after finishing treatment.
-
Living with, through, and beyond thyroid cancer. According to this definition, cancer survivorship begins at diagnosis and continues during treatment and through the rest of a person's life.
For some, the term “survivorship” itself does not feel right, and they may prefer to use different language to describe and define their experience. Sometimes long-term treatment will be used for months or years to manage or control cancer. Living with cancer indefinitely is not easy, and the health care team can help you manage the challenges that come with it . Everyone has to find their own path to name and navigate the changes and challenges that are the results of their cancer diagnosis and treatment.
Survivors may experience a mixture of feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after a cancer diagnosis and have gained a greater acceptance of themselves. Others become very anxious about their health and uncertain about coping with everyday life. Feelings of fear and anxiety may still occur as time passes, but these emotions should not be a constant part of your daily life. If they persist, be sure to talk with a member of your health care team.
Survivors may feel some stress when their frequent visits to the health care team end after completing treatment. Often, relationships built with the cancer care team provide a sense of security during treatment, and people miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, emotional challenges including fear of recurrence, sexual health and fertility concerns, and financial and workplace issues.
Every survivor has individual concerns and challenges. With any challenge, a good first step is being able to recognize your fears and talk about them. Effective coping requires:
-
Understanding the challenge you are facing
-
Thinking through solutions
-
Asking for and allowing the support of others
-
Feeling comfortable with the course of action you choose
Many survivors find it helpful to join an in-person support group or an online community of survivors. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of your health care team, individual counseling, or asking for assistance at the learning resource center of the place where you received treatment.
A new perspective on your health
For many people, survivorship serves as a strong motivator to make lifestyle changes.
People recovering from thyroid cancer are encouraged to follow established guidelines for good health, such as not smoking, limiting alcohol, eating well, exercising regularly, and managing stress. Regular physical activity can help rebuild your strength and energy level. Your health care team can help you create an appropriate exercise plan based upon your needs, physical abilities, and fitness level. Learn more about making healthy lifestyle choices .
It is important to have recommended medical checkups and tests (see Follow-up Care ) to take care of your health. If thyroid hormone replacement is prescribed, it is important to take your medication on schedule, usually daily.
Talk with your health care team to develop a survivorship care plan that is best for your needs.
Changing role of caregivers
Family members and friends may also go through periods of transition. A caregiver plays a very important role in supporting a person diagnosed with cancer, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to the cancer diagnosis will become much less or come to an end. Caregivers can learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about survivorship, explore these related items. Please note that these links will take you to other sections of Cancer.Net:
-
ASCO Answers Guide to Cancer Survivorship: Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. The free booklet is available as a PDF, so it is easy to print.
-
Survivorship Resources: Cancer.Net offers information and resources to help survivors cope, including specific sections for children , teens and young adults , and people over age 65 . There is also a main section on survivorship for people of all ages.
The next section offers Questions to Ask the Health Care Team to help start conversations with your cancer care team. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask your doctor or other members of the health care team, to help you better understand your diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your health care. These suggested questions are a starting point to help you learn more about your cancer care and treatment. You are also encouraged to ask additional questions that are important to you. You may want to print this list and bring it to your next appointment, or download Cancer.Net’s free mobile app for a digital list and other interactive tools to manage your care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask after getting a diagnosis
-
What type of thyroid cancer do I have?
-
Can you explain my pathology report (laboratory test results) to me?
-
What is the stage of the cancer? What does this mean?
-
If medullary thyroid cancer (MTC) is diagnosed, do I need a genetic test? Why or why not? Should family members be tested?
Questions to ask about choosing a treatment and managing side effects
-
What are my treatment options?
-
What types of research are being done for thyroid cancer in clinical trials? Do clinical trials offer additional treatment options for me?
-
What treatment plan do you recommend? Why?
-
What is the goal of each treatment? Is it to eliminate the cancer, help me feel better, or both?
-
What experience do you have in treating this type of thyroid cancer?
-
Where can I get a second opinion?
-
Do I need to make a treatment decision right away?
-
What are the possible side effects of each treatment, both in the short term and the long term?
-
Who will be part of my health care team, and what does each member do?
-
Who will be leading my overall treatment?
-
Will any of these treatments cause hypothyroidism? If so, what can I expect during this time?
-
How will this treatment affect my daily life? Will I be able to work, exercise, or perform my usual activities?
-
Could this treatment affect my sex life? If so, how and for how long?
-
Could this treatment affect my ability to become pregnant or have children? If so, should I talk with a fertility specialist before cancer treatment begins?
-
If I’m worried about the costs of cancer care, who can help me?
-
What support services are available to me? To my family?
-
If I have questions or problems, who should I call?
Questions to ask about surgery
-
Is surgery recommended? If so, how much of my thyroid gland will be removed? Will lymph nodes be removed as well?
-
What type of scar can I expect?
-
Do I need other tests, such as an ultrasound, before surgery to determine the extent of the cancer?
-
How experienced is the surgeon in this type of surgery? How many thyroid surgeries does the surgeon do per week? How many years has the surgeon been performing thyroid surgery?
-
What complications and outcomes have other patients had after being treated by this surgeon?
-
How long will the operation take? How long will I be in the hospital for the surgery?
-
Can you describe what my recovery from surgery will be like?
-
Who should I contact about any side effects I experience? And how soon?
Questions to ask about thyroid hormone therapy
-
Will I need to take thyroid hormone pills before and/or after surgery? If so, for how long?
-
When do I need to start taking thyroid hormone pills?
-
Should I take my pill at the same time each day?
-
What are some ways I can remind myself to take my pill each day?
-
What should I do if I miss taking a pill?
-
Who should I contact about any side effects of hyperthyroidism or hypothyroidism I experience? And how soon?
-
Will my dose be adjusted in the future? How often?
-
What supplements or medications interfere with thyroid hormone replacement?
Questions to ask about radioactive iodine (I-131) treatment
-
Is radioactive iodine treatment recommended? Why or why not? If so, can you describe this procedure to me?
-
Will I need to follow a low-iodine diet before this treatment? If so, when and for how long?
-
Are there precautions I should take after having this treatment?
-
What are the possible side effects of this treatment, in the short term and over time?
-
Who should I contact about any side effects I experience? And how soon?
-
What can be done to prevent or relieve the side effects?
Questions to ask about having other treatments, such as targeted therapy, chemotherapy, or radiation therapy
-
What type of treatment is recommended?
-
What is the goal of this treatment?
-
How long will I have this treatment?
-
Will I receive this treatment at a hospital or clinic? Or will I take it at home?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about planning follow-up care
-
What is the chance that the cancer will come back? Should I watch for specific signs or symptoms?
-
What long-term side effects or late effects are possible based on the cancer treatment I received?
-
If I need to take thyroid hormone replacement, how often do I need my dose checked through blood tests?
-
What follow-up tests will I need, and how often will those tests be needed?
-
Will I need to stop taking thyroid hormone replacement for these tests? If so, for how long and what can I expect during this time?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
When should I return to my primary care doctor for regular medical care?
-
Who will be leading my follow-up care?
-
What survivorship support services are available to me? To my family?
The next section in this guide is Additional Resources . It offers more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Thyroid Cancer - Additional Resources
ON THIS PAGE: You will find some helpful links to other areas of Cancer.Net that provide information about cancer care and treatment. This is the final page of Cancer.Net’s Guide to Thyroid Cancer. Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of cancer for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment, and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Read more about the first steps to take when you are diagnosed with cancer .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of cancer care.
-
Learn more about coping with the emotions that cancer can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for people with thyroid cancer.
-
Explore what to do when you finish active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
Watch Cancer.Net videos with ASCO experts, patients, and caregivers explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
This is the end of Cancer.Net’s Guide to Thyroid Cancer. Use the menu to choose a different section to read in this guide.