













Prostate Cancer - Introduction
ON THIS PAGE: You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Prostate Cancer. Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
About the prostate
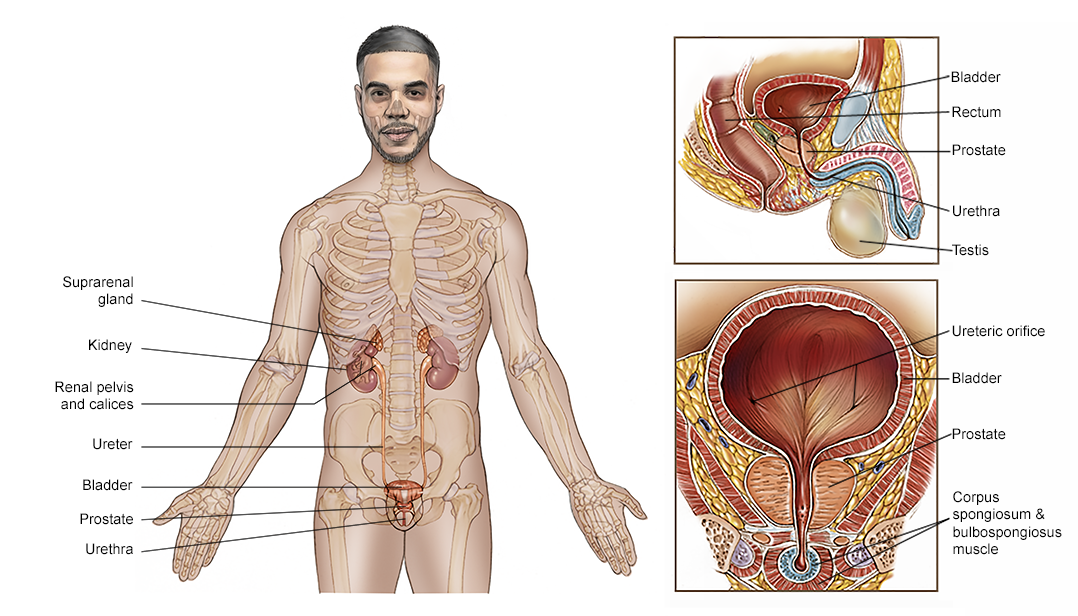
The prostate is a walnut-sized gland located behind the base of the penis, in front of the rectum, and below the bladder. It surrounds the urethra, the tube-like channel that carries urine and semen through the penis. The prostate's main function is to make seminal fluid, the liquid in semen that protects, supports, and helps transport sperm.
The prostate continues to enlarge as people age. This can lead to a condition called benign prostatic hypertrophy (BPH), which is when the urethra becomes blocked. BPH is a common condition associated with growing older, and it has not been associated with a greater risk of having prostate cancer.
About prostate cancer
Cancer begins when healthy cells in the prostate change and grow out of control, forming a tumor. A tumor can be cancerous or benign. A cancerous tumor is malignant, meaning it can grow and spread to other parts of the body. A benign tumor means the tumor can grow but will not spread.
Prostate cancer is somewhat unusual when compared with other types of cancer. This is because many prostate tumors do not spread quickly to other parts of the body. Some prostate cancers grow very slowly and may not cause symptoms or problems for years or ever. Even when prostate cancer has spread to other parts of the body, it often can be managed with treatment for a long time. So people with prostate cancer, and even those with advanced prostate cancer, may live with good health and quality of life for many years. However, if the cancer cannot be well controlled with existing treatments, it can cause symptoms like pain and fatigue and can sometimes lead to death. An important part of managing prostate cancer is watching for growth over time to find out if it is growing slowly or quickly. Based on the pattern of growth, your doctor can decide the best available treatment options and when to give them.
Histology is how cancer cells look under a microscope. The most common histology found in prostate cancer is called adenocarcinoma. Other, less common histologic types, called variants, include neuroendocrine prostate cancer and small cell prostate cancer. These variants tend to be more aggressive, produce much less prostate-specific antigen (PSA), and spread outside the prostate earlier. Read more about neuroendocrine tumors .
About prostate-specific antigen (PSA)
Prostate-specific antigen (PSA) is a protein produced by cells in the prostate gland and released into the bloodstream. PSA levels are measured using a blood test. Although there is no such thing as a “normal PSA” for anyone at any given age, a higher-than-normal level of PSA can be found in people with prostate cancer. Other non-cancerous prostate conditions, such as BPH (see above) or prostatitis can also lead to an elevated PSA level. Prostatitis is the inflammation or infection of the prostate. In addition, some activities like ejaculation can temporarily increase PSA levels. Ejaculations should be avoided before a PSA test to avoid falsely elevated tests. People should discuss with their primary care doctor the pros and cons of PSA testing before using it to screen for prostate cancer. See the Screening section for more information.
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to other sections on Cancer.Net:
-
ASCO Answers Fact Sheet: Read a 1-page fact sheet that offers an introduction to prostate cancer. This free fact sheet is available as a PDF, so it is easy to print.
-
ASCO Answers Guide: Get this free 52-page booklet that helps you better understand the disease and treatment options. The booklet is available as a PDF, so it is easy to print.
-
Cancer.Net En Español: Read about prostate cancer in Spanish or read a 1-page ASCO Answers Fact Sheet in Spanish. Infórmase sobre cáncer de próstata en español o una hoja informativa de una página, Respuestas sobre el cáncer .
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with prostate cancer and general survival rates. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Statistics
ON THIS PAGE: You will find information about the estimated number of people who will be diagnosed with prostate cancer each year. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with cancer are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this cancer and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for you individually. The original sources for these statistics are provided at the bottom of this page.
How many people are diagnosed with prostate cancer?
Prostate cancer is the most common cancer among men, except for skin cancer. In 2023, an estimated 288,300 men in the United States will be diagnosed with prostate cancer. Worldwide, an estimated 1,414,259 people were diagnosed with prostate cancer in 2020. It is the fourth most commonly diagnosed cancer in the world.
Prostate cancer incidence rates dropped steeply from 2007 to 2014 because screening guidelines at the time resulted in less prostate-specific antigen (PSA) testing . But since 2014, overall incidence rates have gone up by around 3% each year, and incidence rates for advanced-stage prostate cancer rose by 5% each year.
Around 60% of cases are diagnosed in people age 65 or older. The average age at the time of diagnosis is 66 years. The disease is rarely identified in those younger than 40. The number of new cases diagnosed in Black men is 70% higher than the number of new cases diagnosed in White men. Black men in the United States and the Caribbean have the highest incidence rates of prostate cancer around the globe.
Prostate cancer is the second leading cause of cancer death in men in the United States. It is estimated that 34,700 deaths from this disease will occur in the United States in 2023. In 2020, an estimated 375,304 people worldwide died from prostate cancer.
However, the death rate dropped by half from 1993 to 2013 as a result of advances in screening and treatment. From 2016 to 2020, the decline in the death rate slowed to just over a half of a percent each year, likely as a result of the increase in prostate cancers diagnosed at an advanced stage. There are more than 3.1 million survivors of prostate cancer in the United States today.
What is the survival rate for prostate cancer?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from prostate cancer. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having cancer may affect life expectancy. Relative survival rate looks at how likely people with prostate cancer are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this cancer.
Example: Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for people with prostate cancer are only an estimate. They cannot tell an individual person if cancer will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for prostate cancer in the United States is 97%. The 10-year relative survival rate is 98%.
The survival rates for prostate cancer vary based on several factors. These include the stage and grade of the cancer, a person’s age and general health, and how well the treatment plan works. Another factor that can affect outcomes is the type of prostate cancer.
Approximately 83% of prostate cancers are found when the disease is in only the prostate and nearby organs (70% local and 13% regional). This is referred to as the local or regional stage. The 5-year relative survival rate for most people with local or regional prostate cancer is nearly 100%. For people diagnosed with prostate cancer that has spread to other parts of the body, the 5-year relative survival rate is 32%.
Experts measure relative survival rate statistics for prostate cancer every 5 years. This means the estimate may not reflect the results of advancements in how prostate cancer is diagnosed or treated from the last 5 years. Talk with your doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's (ACS) publication, Cancer Facts & Figures 2023 , the ACS website, and the International Agency for Research on Cancer website. (All sources accessed March 2023.)
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by prostate cancer. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Medical Illustrations
ON THIS PAGE: You will find a drawing of the main body parts affected by prostate cancer. Use the menu to see other pages.
The next section in this guide is Risk Factors and Prevention . It explains the factors that may increase the chance of developing prostate cancer and what people can do to lower their risk. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Risk Factors and Prevention
ON THIS PAGE: You will find out more about the factors that increase the chance of developing prostate cancer. Use the menu to see other pages.
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the chance to develop cancer, most do not directly or by themselves cause cancer. Some people with several known risk factors never develop cancer, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
The following factors may raise a person's risk of developing prostate cancer:
-
Age. The risk of prostate cancer increases with age, especially after age 50. Around 60% of prostate cancers are diagnosed in people who are 65 or older. Older adults who are diagnosed with prostate cancer can face unique challenges, specifically with regard to cancer treatment. For more information, please visit Cancer.Net’s section about aging and cancer .
-
Race. Black men in the United States, and other men of African ancestry, are diagnosed with prostate cancer more than men of other races. Black men are more likely to die from prostate cancer than White men.
-
North American or northern European location. Prostate cancer occurs most often in North America and northern Europe. It also appears that prostate cancer is increasing among Asian people living in urbanized environments, such as Hong Kong, Singapore, and North American and European cities, particularly among those who have a lifestyle with less physical activity and a less healthy diet.
-
Family history. Prostate cancer that runs in a family, called familial prostate cancer, makes up about 20% of all prostate cancers. This type of prostate cancer develops because of a combination of shared genes and shared environmental or lifestyle factors.
Hereditary prostate cancer, which is inheriting the risk from a relative, is rare and accounts for about 5% of all cases. Hereditary prostate cancer occurs when changes in genes, or mutations, are passed down within a family from 1 generation to the next. This is called a germline mutation. If someone has a first-degree relative—meaning a parent, sibling, or child—with prostate cancer, their risk of developing prostate cancer is 2 to 3 times higher than the average risk. This risk increases even further with the number of relatives diagnosed with prostate cancer.
Hereditary prostate cancer may be suspected if a family history includes any of the following characteristics:-
3 or more first-degree relatives with prostate cancer
-
Prostate cancer in 3 generations on the same side of the family
-
2 or more close relatives, such as a parent, sibling, child, grandparent, uncle, or nephew, on the same side of the family diagnosed with prostate cancer before age 55
-
-
Hereditary breast and ovarian cancer (HBOC) syndrome. HBOC is associated with germline, or inherited, DNA-repair mutations to the BRCA1 and/or BRCA2 genes. BRCA stands for “BReast CAncer.” HBOC is most commonly associated with an increased risk of breast and ovarian cancers in women. However, men with HBOC also have an increased risk of developing breast cancer and a more aggressive form of prostate cancer. Mutations in the BRCA1 and BRCA2 genes are thought to cause only a small percentage of inherited prostate cancers. Those who have BRCA1 or BRCA2 mutations should consider screening for prostate cancer at an earlier age. Genetic testing may only be appropriate for families with prostate cancer that may also have HBOC. If you are concerned about this based on your own family history, please talk with a genetic counselor or doctor for more information.
-
Other genetic changes. Other genes that may carry an increased risk of developing prostate cancer include HPC1 , HPC2 , HPCX , CAPB , ATM , FANCA , HOXB13 , and mismatch repair genes. However, none of them has been directly shown to cause prostate cancer or be specific to this disease. Research to identify genes associated with an increased risk of prostate cancer is ongoing, and researchers are constantly learning more about how specific genetic changes can influence the development of prostate cancer. At present, there are no genetic tests available to determine someone's chance of developing prostate cancer.
-
Agent Orange exposure. The U.S. Department of Veterans Affairs (VA) lists prostate cancer as a disease associated with exposure to Agent Orange, a chemical used during the Vietnam War. If you are a veteran who may have been exposed to Agent Orange, please talk to your doctor in the VA system. Learn more about the link with Agent Orange in this article .
-
Eating habits and weight. No study has proven that diet and nutrition can directly cause or prevent the development of prostate cancer. However, many studies that look at links between certain eating behaviors and cancer suggest there may be a connection. For example, obesity is associated with many cancers , including prostate cancer, and a healthy diet to avoid weight gain is recommended (see “Dietary changes” below).
Prevention
Different factors cause different types of cancer. Researchers continue to look into what factors cause prostate cancer, including ways to prevent it. Although there is no proven way to completely prevent prostate cancer, you may be able to lower your risk. Talk with your health care team for more information about your personal risk of cancer.
Chemoprevention
A class of drugs called 5-alpha-reductase inhibitors (5-ARIs), which includes dutasteride (Avodart) and finasteride (Proscar), are often used to treat benign prostatic hypertrophy (BPH). They may also lower the risk of developing prostate cancer. Some previous clinical trials suggested that 5-ARIs were linked to more aggressive prostate cancers, but newer studies have suggested that this is not true. According to the results of a long-term follow-up study published in 2013, 78% of people either taking finasteride or a placebo were still alive 15 years later. These results suggest that taking finasteride does not lower the risk of death for those with prostate cancer. The U.S. Food and Drug Administration (FDA) has not approved these drugs for the prevention of prostate cancer. However, a 5-ARI is approved by the FDA for the treatment of lower urinary tract symptoms associated with BPH.
The decision to take a 5-ARI is different for each person. Anyone considering taking this class of medication should discuss the possible benefits and side effects with their doctor.
Dietary changes
There is not enough information right now to make clear recommendations about the exact role eating behaviors play in prostate cancer. Dietary changes may need to be made many years earlier in a person’s life to reduce the risk of developing prostate cancer later in life.
Here is a brief summary of the current research:
-
In some studies, regularly eating foods high in fat, especially animal fat, has been associated with increased prostate cancer risk. However, no prospective studies have yet proven that diets high in animal fat raise the risk of prostate cancer. Prospective studies look at people who follow either high-fat or low-fat diets and then measure the total number of people in each group who are diagnosed with prostate cancer.
-
A diet high in vegetables, fruits, and legumes, such as beans and peas, may lower the risk of prostate cancer. It is unclear which nutrients are directly responsible. Although lycopene, a nutrient found in tomatoes and other vegetables, has been shown to be associated with a lower risk of prostate cancer, the data have not proven that there is a relationship between lycopene and preventing cancer.
-
Currently no specific vitamins, minerals, or other supplements have been shown in clinical trials to prevent prostate cancer. Talk with your doctor before taking any supplements to prevent prostate cancer.
-
Specific changes to eating behaviors may not stop or slow the development of prostate cancer. It is possible such changes would need to be made early in life to have an effect.
The next section in this guide is Screening . It explains how tests may find cancer before signs or symptoms appear. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Screening
ON THIS PAGE: You will find out more about screening for prostate cancer. You will also learn the risks and benefits of screening. Use the menu to see other pages.
Screening is used to look for cancer before you have any symptoms or signs. When cancer is found earlier in its development, it is often at an earlier stage. This means that there is a better chance of successfully treating the cancer. Scientists have developed, and continue to develop, tests that can be used to screen a person for specific types of cancer. The overall goals of cancer screening are to:
-
Lower the number of people who die from the disease, or eliminate deaths from cancer altogether
-
Lower the number of people who develop the disease
Learn more about the basics of cancer screening .
Screening information for prostate cancer
Screening for prostate cancer is done to find evidence of cancer in otherwise healthy adults. Two tests are commonly used to screen for prostate cancer:
Digital rectal examination (DRE)
A DRE is a test in which the doctor inserts a gloved, lubricated finger into the rectum and feels the surface of the prostate through the bowel wall for any irregularities.
Prostate-specific antigen (PSA) blood test
There is controversy about using the PSA test to look for prostate cancer in people with no symptoms of the disease. On the one hand, the PSA test is useful for detecting early-stage prostate cancer, especially in those with many risk factors, which helps some get the treatment they need before the cancer grows and spreads. On the other hand, PSA screening may find very-slow-growing prostate cancers that would never threaten someone's life. As a result, screening for prostate cancer using PSA may lead to treatments that are not needed, which can cause side effects and seriously affect a person's quality of life.
ASCO recommends that people with no symptoms of prostate cancer and who are expected to live less than 10 years do not receive PSA screening. For those expected to live longer than 10 years, ASCO recommends that they talk with their doctor to find out if the test is appropriate for them.
Other organizations have different recommendations for screening:
-
The U.S. Preventive Services Task Force (USPSTF) recommends that adults between 55 and 69 should discuss the pros and cons of PSA screening with their doctor before making a decision about screening. People who are 70 and older should not have routine PSA screenings for prostate cancer.
-
The American Urological Association and the American Cancer Society recommend that people be told the risks and benefits of testing before PSA screening occurs and then make an informed decision in consultation with their doctor.
-
The National Comprehensive Cancer Network (NCCN) considers a patient’s age, PSA value, DRE results, and other factors in their recommendations. Based on those risk factors and test results, repeat screening tests may be recommended every 2 to 4 years or 1 to 2 years.
It is not easy to predict which tumors will grow and spread quickly and which will grow slowly. Everyone should discuss with their doctor the pros and cons of prostate cancer screening based on their situation and personal risk of prostate cancer, so they can work together to make an informed decision.
The next section in this guide is Symptoms and Signs . It explains what body changes or medical problems prostate cancer can cause. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Symptoms and Signs
ON THIS PAGE: You will find out more about changes and other things that can signal a problem that may need medical care. Use the menu to see other pages.
Symptoms are changes that you can feel in your body. Signs are changes in something measured, like by taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem. While most prostate cancer does not cause any symptoms, the symptoms and signs of prostate cancer may include:
-
Frequent urination
-
Weak or interrupted urine flow or the need to strain to empty the bladder
-
The urge to urinate frequently at night
-
Blood in the urine
-
New onset of erectile dysfunction
-
Pain or burning during urination, which is much less common
-
Discomfort or pain when sitting, caused by an enlarged prostate
Other noncancerous conditions of the prostate, such as benign prostatic hypertrophy (BPH) or an enlarged prostate, can cause similar symptoms. Or, the cause of a symptom or sign may be another medical condition that is also not related to cancer. Urinary symptoms also can be caused by an infection of the bladder or other conditions.
If cancer has spread outside of the prostate gland, symptoms and signs may include:
-
Pain in the back, hips, thighs, shoulders, or other bones
-
Swelling or fluid buildup in the legs or feet
-
Unexplained weight loss
-
Fatigue
-
Change in bowel habits
If you are concerned about any changes you experience, please talk with your doctor. Your doctor will ask how long and how often you have been experiencing the symptom(s), in addition to other questions. This is to help figure out the cause of the problem, called a diagnosis.
If cancer is diagnosed, relieving symptoms remains an important part of cancer care and treatment. Managing symptoms may be called "palliative care" or "supportive care." It is often started soon after diagnosis and continued throughout treatment. Be sure to talk with your health care team about the symptoms you experience, including any new symptoms or a change in symptoms.
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Diagnosis
ON THIS PAGE: You will find a list of common tests, procedures, and scans that doctors use to find the cause of a medical problem. Use the menu to see other pages.
Doctors use many tests to find, or diagnose, cancer. They also do tests to learn if cancer has spread to another part of the body from where it started. If the cancer has spread, it is called metastasis. Doctors may also do tests to learn which treatments could work best.
For most types of cancer, a biopsy is the only sure way for the doctor to know if an area of the body has cancer. In a biopsy, the doctor takes a small sample of tissue for testing in a laboratory.
How prostate cancer is diagnosed
There are many tests used for diagnosing prostate cancer. Not all tests described here are commonly used for every person. Your doctor may consider these factors when choosing a diagnostic test:
-
The type of cancer suspected
-
Your signs and symptoms
-
Your age and general health
-
The results of earlier medical tests
Early tests
If prostate cancer is suspected, a physical examination and the following tests may be used to decide if more diagnostic tests are needed:
Prostate-specific antigen (PSA) test. As described in the Introduction and Screening sections, PSA is a protein released by prostate tissue that is found in higher levels in blood. Levels can be raised when there is abnormal activity in the prostate, including prostate cancer, benign prostatic hypertrophy (BPH), or inflammation of the prostate. Doctors can look at features of the PSA value to decide if a biopsy is needed, such as absolute level, change over time (also known as “PSA velocity”), and level in relation to prostate size.
Free PSA test. There is a version of the PSA test that allows the doctor to measure a specific component, called the “free” PSA. Free PSA is found in the bloodstream and is not bound to proteins. A standard PSA test measures total PSA, which includes both PSA that is and is not bound to proteins. The free PSA test measures the ratio of free PSA to total PSA. Knowing this ratio or percent can sometimes help find out if an elevated PSA level is more likely to be associated with a malignant condition like prostate cancer.
Digital rectal exam (DRE). A doctor uses a DRE to find abnormal parts of the prostate by feeling the area using a finger. It is not very precise and not every doctor has expertise in the technique; therefore, DRE does not usually detect early prostate cancer. See the Screening section for more information.
Biomarker tests. A biomarker is a substance that is found in the blood, urine, or body tissues of a person with cancer. It is made by the tumor or by the body in response to the cancer. A biomarker may also be called a tumor marker. Biomarker tests for prostate cancer include the 4Kscore, which predicts the chances someone has high-risk prostate cancer, and the Prostate Health Index (PHI), which predicts the chances someone has prostate cancer.
For people diagnosed with prostate cancer by biopsy, there are times when a genomic test, such as Oncotype Dx Prostate, Prolaris, Decipher, and ProMark, can provide additional information to inform a decision about how the prostate cancer is managed. This includes when people with certain low-risk or intermediate-risk localized prostate cancer are considering active surveillance (see
Types of Treatment
). It also may include using the Decipher test to help decide whether more treatment should be considered in certain patients following surgical removal of the prostate, called prostatectomy. If a biomarker test is used, the results should always be evaluated in combination with all other available information.
Talk with your doctor for more information about biomarker tests, what they mean, and how the results might or might not affect your treatment plan.
This information is based on the ASCO guideline, "
Molecular Biomarkers in Localized Prostate Cancer
." Please note that this link takes you to a different ASCO website.
Making a diagnosis
If the PSA or DRE test results are abnormal, then further tests will be used to confirm whether a person has prostate cancer. Many tests can suggest that cancer is present, but only a biopsy can make a definite diagnosis.
Biopsy. A biopsy is the removal of a small amount of tissue for examination under a microscope. To get a tissue sample, a surgeon most often uses transrectal ultrasound (TRUS, see below) and a biopsy tool to take very small slivers of prostate tissue. Biopsy specimens will be taken from several areas of the prostate. This is done to make sure that a good sample is taken for examination. Most people will have 12 to 14 pieces of tissue removed, and the procedure can take 20 to 30 minutes to complete.
This procedure is usually done at the hospital or doctor’s office without needing to stay overnight. The patient is given local anesthesia beforehand to numb the area and usually receives antibiotics before the procedure to prevent infection. The ultrasound tool is inserted into the rectum and then the biopsy needle is passed through the rectum and into the prostate gland to collect tissue samples.
There is a risk of infection associated with transrectal prostate biopsy, which is why some doctors choose to use transperineal prostate biopsy instead. This biopsy is also guided by TRUS, but the biopsy needle goes through the skin of the perineum and into the prostate gland. The perineum is the space between the scrotum and the anus. By passing the needle through the skin instead of the rectum, this procedure lowers the risk of infection.
A pathologist then analyzes the sample(s) under a microscope. A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease.
Ask to review the results of the pathology report with your health care team.
MRI fusion biopsy. An MRI fusion biopsy combines magnetic resonance imaging (MRI, see below) with TRUS. Evaluation with a prostate MRI scan has become a routine procedure in clinical practice. The patient first receives an MRI scan to identify suspicious areas of the prostate that require further evaluation. The patient then has an ultrasound of the prostate. Computer software combines these images to produce a 3-dimensional image that helps target a precise area for the biopsy. Although it may not eliminate the need for repeat biopsies, an MRI fusion biopsy can better identify areas that are more likely to be cancerous than other methods. An MRI fusion biopsy should only be performed by someone with expertise in the procedure.
Transrectal ultrasound (TRUS). A doctor inserts a probe into the rectum that takes a picture of the prostate using sound waves that bounce off the prostate. A TRUS is usually done at the same time as a biopsy.
Finding out if the cancer has spread ( updated 11/2023)
To find out if cancer has spread outside of the prostate, doctors may perform the imaging tests listed below. Doctors are able to estimate the risk of spread, called metastasis, based on PSA levels, tumor grade, and other factors, but an imaging test can confirm and provide information about the cancer’s location. Imaging tests show pictures of the inside of the body.
Imaging tests may not always be needed. A computed tomography (CT) scan or bone scan may not be necessary for those with no symptoms and low-risk, early-stage prostate cancer, as determined with information from the PSA test and biopsy. Learn more about when these tests are recommended to find out if the cancer has spread .
For people with advanced prostate cancer, ASCO recommends that 1 or more of the imaging tests below be done to provide more information about the disease and help plan the best treatment. This includes when there is a newly diagnosed, high-risk cancer; if metastasis is suspected or confirmed; if the cancer has returned following treatment; or when the cancer grows during the treatment period. Learn more about this guideline on the ASCO website.
Whole-body bone scan. A bone scan uses a radioactive tracer (Technetium-99) to look at the inside of the bones. The amount of radiation in the tracer is too low to be harmful. The tracer is injected into a patient’s vein. It collects in areas of the bone where metabolic activity has occurred. Healthy bone appears lighter to the camera, and areas of injury, such as those caused by cancer, stand out on the image. It is important to know that structural changes to the bone, such as arthritis or bone injuries like fractures, can also be interpreted as abnormal and need to be evaluated by a doctor to make sure they are not cancer.
Computed tomography (CT or CAT) scan. A CT scan takes pictures of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed, 3-dimensional image that shows any abnormalities or tumors. A CT scan can be used to measure the tumor’s size. Sometimes, a special dye called a contrast medium is given before the scan to provide better detail on the image. This dye can be injected into a patient’s vein or given as a pill or liquid to swallow.
Magnetic resonance imaging (MRI). An MRI scan uses magnetic fields, not x-rays, to produce detailed images of the body. An MRI can be used to measure the tumor’s size, and a scan can focus specifically on the area of the prostate or on the whole body. A special dye called contrast medium is given before the scan to create a clearer picture, which is injected into a patient’s vein.
Positron emission tomography (PET) or PET-CT scan. A PET scan is usually combined with a CT scan (see above), called a PET-CT scan . However, you may hear your doctor refer to this procedure just as a PET scan. A PET scan is a way to create pictures of organs and tissues inside the body. A small amount of a radioactive substance is injected into the patient’s body. This substance is taken up by cells that use the most energy or are more biologically active. Because cancer tends to use energy and is biologically active, it absorbs more of the radioactive substance. However, the amount of radiation in the substance is too low to be harmful. A scanner then detects this substance to produce images of the inside of the body.
For many types of cancer, a PET-CT scan uses fluorodeoxyglucose (FDG) as the substance that is imaged; however, FDG is not a useful substance for initial imaging in prostate cancer and should not be routinely used. If metastasis or recurrence are suspected, a PET scan using gallium-68 or fluorine-18 may be recommended. In this type of scan, the gallium-68 or fluorine-18 binds to prostate-specific membrane antigen (PSMA), which is often at higher levels in prostate cancer cells, and shows places where the cancer has spread.
Researchers are investigating using different substances with PET scans to find prostate cancer. For example, sodium fluoride is absorbed by bones, and its use in a PET scan may improve the chances of finding prostate cancer that has spread to the bone. Other substances being studied include choline acetate and fluciclovine.
After diagnostic tests are done, your doctor will review the results with you. If the diagnosis is cancer, these results also help the doctor describe the cancer. This is called staging.
The next section in this guide is Stages and Grades . It explains the system doctors use to describe the extent of the disease and how the cancer cells look under a microscope. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Stages and Grades
ON THIS PAGE: You will learn about how doctors describe a cancer’s growth or spread, as well as what the cancer cells look like under a microscope. This is called the stage and grade. Use the menu to see other pages.
What is cancer staging?
Staging is a way of describing where the cancer is located, if or where it has spread, and whether it is affecting other parts of the body.
Doctors use diagnostic tests to find out the cancer's stage, so staging may not be complete until all of the tests are finished. Staging for prostate cancer also involves looking at test results to find out if the cancer has spread from the prostate to other parts of the body. Knowing the stage helps the doctor recommend the best kind of treatment, and it can help predict a patient's prognosis, which is the chance of recovery. There are different stage descriptions for different types of cancer.
There are 2 types of staging for prostate cancer:
-
Clinical staging. This is based on the results of a digital rectal exam (DRE), prostate-specific antigen (PSA) testing, and Gleason score (see “Gleason score for grading prostate cancer” below). These test results will help determine whether x-rays, bone scans, computed tomography (CT) scans, or magnetic resonance imaging (MRI) are also needed. If scans are needed, they can add more information to help the doctor figure out the clinical stage.
-
Pathologic staging. This is based on information found during surgery, plus the laboratory results of the prostate tissue removed during surgery, also called the pathology. The surgery often includes the removal of the entire prostate and some lymph nodes. Examination of the removed lymph nodes can provide more information for pathologic staging.
This page provides detailed information about the system used to find the stage of prostate cancer and the stage groups for prostate cancer, such as stage II or stage IV.
-
TNM staging system
-
Gleason score for grading prostate cancer
-
Stage groups for prostate cancer
-
Prostate cancer risk groups
TNM staging system
One tool that doctors use to describe the stage is the TNM system. This system is developed by the American Joint Committee on Cancer. Doctors use the results from diagnostic tests and scans to answer these questions:
-
Tumor (T): How large is the primary tumor? Where is it located?
-
Node (N): Has the tumor spread to the lymph nodes? If so, where and how many? Lymph nodes are small, bean-shaped organs that help fight infection.
-
Metastasis (M): Has the cancer spread to other parts of the body? If so, where and how much?
The results are combined to determine the stage of cancer for each person. There are 5 stages: stage 0 (zero) and stages I through IV (1 through 4). The stage provides a common way of describing the cancer, so doctors can work together to plan the best treatments.
Return to top
Gleason score for grading prostate cancer
Prostate cancer is also given a grade called a Gleason score. This score is based on how much the cancer looks like healthy tissue when viewed under a microscope. Less aggressive tumors generally look more like healthy tissue. Tumors that are more aggressive are likely to grow and spread to other parts of the body. They look less like healthy tissue.
The Gleason scoring system is the most common prostate cancer grading system used. The pathologist looks at how the cancer cells are arranged in the prostate and assigns a score on a scale of 3 to 5 from 2 different locations. Cancer cells that look similar to healthy cells receive a low score. Cancer cells that look less like healthy cells or look more aggressive receive a higher score. To assign the numbers, the pathologist determines the main pattern of cell growth, which is the area where the cancer is most obvious and then looks for another area of growth. The doctor then gives each area a score from 3 to 5. The scores are added together to come up with an overall score between 6 and 10.
Overall, Gleason scores of 5 or lower are not used. The lowest Gleason score is 6, which is a low-grade cancer. A Gleason score of 7 is a medium-grade cancer, and a score of 8, 9, or 10 is a high-grade cancer. A lower-grade cancer grows more slowly and is less likely to spread than a high-grade cancer.
Doctors look at the Gleason score in addition to stage to help plan treatment. For example, active surveillance (see Types of Treatment ) may be an option for someone with a small tumor, low PSA level, and a Gleason score of 6. People with a higher Gleason score may need treatment that is more intensive, even if the cancer is not large or has not spread.
-
Gleason X: The Gleason score cannot be determined.
-
Gleason 6 or lower: The cells look similar to healthy cells, which is called well differentiated.
-
Gleason 7: The cells look somewhat similar to healthy cells, which is called moderately differentiated.
-
Gleason 8, 9, or 10: The cells look very different from healthy cells, which is called poorly differentiated or undifferentiated.
Return to top
Stage groups for prostate cancer
Doctors assign combine the T, N, and M information to say what stage the cancer is. Staging also includes the PSA level (see Screening ) and Gleason score.
Stage I: Cancer in this early stage is usually slow growing. The tumor cannot be felt and involves one-half of 1 side of the prostate or even less than that. PSA levels are low. The cancer cells look like healthy cells.
Stage II: The tumor is found only in the prostate. PSA levels are medium or low. Stage II prostate cancer is small but may have an increasing risk of growing and spreading.
-
Stage IIA: The tumor cannot be felt and involves half of 1 side of the prostate or even less than that. PSA levels are medium, and the cancer cells are well differentiated. This stage also includes larger tumors found only in the prostate, as long as the cancer cells are still well differentiated.
-
Stage IIB: The tumor is found only inside the prostate, and it may be large enough to be felt during a DRE. The PSA level is medium. The cancer cells are moderately differentiated.
-
Stage IIC: The tumor is found only inside the prostate, and it may be large enough to be felt during a DRE. The PSA level is medium. The cancer cells may be moderately or poorly differentiated.
Stage III: PSA levels are high, the tumor is growing, or the cancer is high grade. These all indicate a locally advanced cancer that is likely to grow and spread.
-
Stage IIIA: The cancer has spread beyond the outer layer of the prostate into nearby tissues. It may also have spread to the seminal vesicles. The PSA level is high.
-
Stage IIIB: The tumor has grown outside of the prostate gland and may have invaded nearby structures, such as the bladder or rectum.
-
Stage IIIC: The cancer cells across the tumor are poorly differentiated, meaning they look very different from healthy cells.
Stage IV: The cancer has spread beyond the prostate.
-
Stage IVA: The cancer has spread to the regional lymph nodes.
-
Stage IVB: The cancer has spread to distant lymph nodes, other parts of the body, or to the bones.
Recurrent: Recurrent prostate cancer is cancer that has come back after treatment. It may come back in the prostate area again or in other parts of the body. If the cancer does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis .
Used with permission of the American College of Surgeons, Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Eighth Edition (2017), published by Springer International Publishing.
Return to top
Prostate cancer risk groups
In addition to stage, doctors may use other prognostic factors to help plan the best treatment and predict how successful treatment will be. Examples of these include the National Comprehensive Cancer Network (NCCN) risk group categories and the Cancer of the Prostate Risk Assessment (CAPRA) risk score from University of California, San Francisco.
Return to top
Information about the cancer’s stage and other prognostic factors will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment . Use the menu to choose a different section to read in this guide.
Prostate Cancer - Types of Treatment
ON THIS PAGE: You will learn about the different types of treatments doctors use for people with prostate cancer. Use the menu to see other pages.
This section explains the types of treatments, also known as therapies, that are the standard of care for prostate cancer. “Standard of care” means the best treatments known. When making treatment plan decisions, you are encouraged to discuss with your doctor whether clinical trials are an option. A clinical trial is a research study that tests a new approach to treatment. Doctors learn through clinical trials whether a new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option for all stages of cancer. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
How prostate cancer is treated
In cancer care, different types of doctors—including medical oncologists, surgeons, and radiation oncologists—often work together to create an overall treatment plan that may combine different types of treatments to treat the cancer. This is called a multidisciplinary team . Cancer care teams include a variety of other health care professionals, such as palliative care experts, physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, dietitians, physical therapists, and others.
Treatment options and recommendations depend on several factors, including the type and stage of cancer, possible side effects, and the patient’s preferences and overall health.
Cancer treatment can affect adults who are 65 and older in different ways. More information on the specific effects of surgery, chemotherapy, and radiation therapy on these patients can be found another section of this website .
Take time to learn about your treatment options and be sure to ask questions if something is unclear. Talk with your doctor about the goals of each treatment, the likelihood that the treatment will work, what you can expect while receiving the treatment, and the possible urinary, bowel, sexual, and hormone-related side effects of treatment . Discuss with your doctor how the treatment options may affect recurrence, survival, and quality of life. It is also important to discuss your doctor's experience with treating prostate cancer. These types of talks are called "shared decision-making." Shared decision-making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision-making is particularly important for prostate cancer because there are different treatment options. Learn more about making treatment decisions .
Because most prostate cancers are found in the early stages when they are growing slowly, you usually do not have to rush to make treatment decisions. During this time, it is important to talk with your doctor about the risks and benefits of all your treatment options and when treatment should begin. This discussion should also address the current state of the cancer:
-
Whether you have symptoms or prostate-specific antigen (PSA) levels are rising rapidly
-
Whether the cancer has spread to the bones
-
Your health history
-
Your quality of life
-
Your current urinary and sexual function
-
Any other medical conditions you may have
Although your treatment recommendations will depend on these factors, there are some general steps for treating prostate cancer by stage. These are described in "Treatments by stage of prostate cancer," further down this page.
The common types of treatments used for prostate cancer are described below. Your care plan may also include treatment for symptoms and side effects, an important part of cancer care.
-
Active surveillance and watchful waiting
-
Surgery
-
Radiation therapy
-
Focal therapies
-
Androgen-deprivation therapy (hormonal therapy)
-
Targeted therapy
-
Chemotherapy
-
Immunotherapy
-
Radiation therapy by infusion
-
Bone-modifying drugs
-
Physical, emotional, and social effects of cancer
-
Early-stage prostate cancer (stages I and II)
-
Locally advanced prostate cancer (stage III)
-
Advanced prostate cancer (stage IV)
-
Remission and the chance of recurrence
-
If treatment does not work
Active surveillance and watchful waiting
If prostate cancer is in an early stage, is growing slowly, and treating the cancer would cause more problems than the disease itself, a doctor may recommend active surveillance or watchful waiting.
Active surveillance. Prostate cancer treatments may seriously affect a person's quality of life. These treatments can cause side effects, such as erectile dysfunction , which is the inability to get and maintain an erection of the penis, and incontinence , which is when urine flow or bowel function cannot be controlled. In addition, many prostate cancers grow slowly and cause no symptoms or problems. For this reason, many people may consider delaying cancer treatment rather than starting treatment right away. This is an approach called active surveillance. During active surveillance, the cancer is closely monitored for signs that it is worsening. If the cancer is found to be worsening, treatment will begin.
Active surveillance is usually preferred for those with very-low-risk and low-risk prostate cancer that can be treated with surgery or radiation therapy if it shows signs of getting worse. ASCO endorses recommendations from CancerCare Ontario on active surveillance, which recommend active surveillance for most patients with cancer that has not spread beyond the prostate, with a Gleason score of 6 or below. Sometimes, active surveillance may be an option for prostate cancer with a Gleason score of 7. There is also growing use of genomic testing to help find out if active surveillance is the best choice for a person with prostate cancer (see more in Latest Research ).
ASCO encourages the following testing schedule for active surveillance:
-
A PSA test every 3 to 6 months
-
A digital rectam exam (DRE) at least once every year
-
Another prostate biopsy within 6 to 12 months, then a biopsy at least every 2 to 5 years
Treatment should begin if the results of the tests done during active surveillance show signs of the cancer becoming more aggressive or spreading, if the cancer causes pain, or if the cancer blocks the urinary tract.
Watchful waiting. Watchful waiting is an approach that may be an option for older adults and those with other serious or life-threatening illnesses who are expected to live less than 5 years. With watchful waiting, routine PSA tests, DRE, and biopsies are not usually done. If the prostate cancer causes symptoms, such as pain or blockage of the urinary tract, then treatment may be recommended to relieve those symptoms. This may include hormonal therapy (see below). Patients who start on active surveillance who later have a shorter life expectancy may switch to watchful waiting at some point to avoid repeated tests and biopsies.
Doctors must collect as much information as possible about the patient’s other illnesses and life expectancy to determine whether active surveillance or watchful waiting is appropriate for each person. In addition, many doctors recommend a repeat biopsy shortly after diagnosis to confirm that the cancer is in an early stage and growing slowly before considering active surveillance for someone who is otherwise healthy. New information is becoming available all the time, and it is important to discuss these issues with the doctor to make the best decisions about treatment. Learn more about ASCO’s endorsement of recommendations for active surveillance on a different ASCO website.
Return to top
Local treatments
Local treatments get rid of cancer from a specific, limited area of the body. Such treatments include surgery and radiation therapy. For early-stage prostate cancer, local treatments may get rid of the cancer completely. If the cancer has spread outside the prostate gland, other types of treatment (such as medications) may be needed to destroy cancer cells located in other parts of the body.
Surgery
Surgery involves the removal of the prostate and some surrounding lymph nodes during an operation. A surgical oncologist is a doctor who specializes in treating cancer using surgery. For prostate cancer, a urologist or urologic oncologist is the surgical oncologist involved in treatment. The type of surgery depends on the stage of the disease, the patient’s overall health, and other factors.
-
Radical (open) prostatectomy. A radical prostatectomy is the surgical removal of the entire prostate and the seminal vesicles. Lymph nodes in the pelvic area may also be removed. This operation has the risk of affecting sexual function. Nerve-sparing surgery, when possible, increases the chance that the patient can maintain sexual function after surgery by avoiding surgical damage to the nerves that allow erections and orgasm to occur. Orgasm can occur even if some nerves are cut because these are separate processes. Urinary incontinence is also a possible side effect of radical prostatectomy. To help resume normal sexual function, drugs, penile implants, or injections may be recommended. Sometimes, another surgery can fix urinary incontinence.
-
Robotic or laparoscopic prostatectomy. This type of surgery is less invasive than a radical prostatectomy and may shorten recovery time. A camera and instruments are inserted through small keyhole incisions in the patient’s abdomen. The surgeon then directs the robotic instruments to remove the prostate gland. In general, robotic prostatectomy causes less bleeding and less pain, but the sexual and urinary side effects are similar to those of a radical (open) prostatectomy. Talk with your doctor about whether your treatment center offers this procedure and how it compares with the results of the radical (open) prostatectomy.
-
Bilateral orchiectomy. Bilateral orchiectomy is the surgical removal of both testicles. It is described in detail in “Hormonal therapy” below.
-
Transurethral resection of the prostate (TURP). TURP is most often used to relieve symptoms of a urinary blockage, not to treat prostate cancer. In this procedure, with the patient under full anesthesia, which is medication to block the awareness of pain, a surgeon inserts a narrow tube with a cutting device called a cystoscope into the urethra and then into the prostate to remove prostate tissue.
Before surgery, talk with your health care team about the possible side effects from the specific surgery you will have. Typically, younger or healthier patients may benefit more from a prostatectomy. Younger patients are also less likely to develop permanent erectile dysfunction and urinary incontinence after a prostatectomy than older patients. Learn more about coping with the sexual side effects of prostate cancer in the Coping With Treatment section.
Learn more about the basics of cancer surgery .
Return to top
Radiation therapy
Radiation therapy is the use of high-energy rays to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
External-beam radiation therapy. External-beam radiation therapy is the most common type of radiation treatment. The radiation oncologist uses a machine located outside the body to focus a beam of x-rays on the area with the cancer.
One method of external-beam radiation therapy used to treat prostate cancer is called hypofractionated radiation therapy. This is when a person receives a higher daily dose of radiation therapy given over a shorter period, instead of lower doses given over a longer period. Extreme hypofraction radiation therapy is when the entire treatment is delivered in 5 or fewer treatments. Moderate hypofraction radiation therapy regimens typically include 20 to 28 treatments. This is also called stereotactic body radiation therapy (SBRT) or stereotactic ablative radiation therapy (SABR).
According to recommendations from ASCO, the American Society for Radiation Oncology, and the American Urological Association, hypofractionated radiation therapy may be an option for the following people with early-stage prostate cancer that has not spread to other parts of the body:
-
People with low-risk prostate cancer who need or prefer treatment instead of active surveillance.
-
People with intermediate-risk or high-risk prostate cancer receiving external-beam radiation therapy to the prostate and possibly the pelvic lymph nodes.
People who receive hypofractionated radiation therapy may have a slightly higher risk of some short-term side effects after treatment compared with those who receive regular external-beam radiation therapy. This may include gastrointestinal side effects. Based on current research, people who receive hypofractionated radiation therapy are not at a higher risk of side effects in the long term. Talk with your health care team if you have questions about your risk for side effects.
Learn more about these recommendations for hypofractionated radiation therapy for prostate cancer on a different ASCO website.
Brachytherapy. Brachytherapy, or internal radiation therapy, is the insertion of radioactive sources directly into the prostate. These sources, called seeds, give off radiation just around the area where they are inserted and may be left for a short time (high-dose rate) or for a longer time (low-dose rate). Low-dose-rate seeds are left in the prostate permanently and work for up to 1 year after they are inserted. However, how long they work depends on the source of radiation. High-dose-rate brachytherapy is usually left in the body for less than 30 minutes, but it may need to be given more than once.
Brachytherapy may be used with other treatments, such as external-beam radiation therapy and/or hormonal therapy. ASCO recommends the following brachytherapy options:
-
People with low-risk prostate cancer who need or choose an active treatment may consider low-dose-rate brachytherapy. Other options include external-beam radiation therapy or a radical prostatectomy.
-
People with intermediate-risk prostate cancer who choose external-beam radiation therapy (with or without hormonal therapy) should be offered either a low-dose-rate or high-dose-rate brachytherapy boost in addition to the external-beam radiation therapy. For a brachytherapy boost, a lower dose of radiation is given for a shorter period of time. Some patients with intermediate-risk prostate cancer may be able to receive only brachytherapy without external-beam radiation therapy or hormonal therapy.
-
Patients with high-risk prostate cancer who are receiving external-beam radiation therapy and hormonal therapy should be offered a low-dose-rate or high-dose-rate brachytherapy boost.
Read ASCO’s recommendations for brachytherapy for prostate cancer , found on a different ASCO website.
Intensity-modulated radiation therapy (IMRT). IMRT is a type of external-beam radiation therapy that uses computed tomography (CT) scans to form a 3D picture of the prostate before treatment. A computer uses this information about the size, shape, and location of the prostate cancer to determine how much radiation is needed to destroy it. With IMRT, high doses of radiation can be directed at the prostate without increasing the risk of damaging nearby organs.
Proton therapy. Proton therapy, also called proton beam therapy, is a type of external-beam radiation therapy that uses protons rather than x-rays. At high energy, protons can destroy cancer cells. Current research has not shown that proton therapy provides any more benefit to people with prostate cancer than traditional radiation therapy. It can also be more expensive.
Side effects of radiation therapy
Radiation therapy may cause side effects during treatment, including increased urge to urinate or frequency of urination; problems with sexual function; problems with bowel function, including diarrhea, rectal discomfort, or rectal bleeding; and fatigue. Most of these side effects usually go away after treatment.
To help support a patient's sexual functioning, drugs, penile implants, or injections may be recommended. Learn more about coping with the sexual side effects of prostate cancer in the Coping With Treatment section. While uncommon, some side effects of radiation therapy may not show up until years after treatment. See Follow-up Care for more information about long-term side effects.
Learn more about the basics of radiation therapy and what to expect when having radiation therapy .
Return to top
Focal therapies
Focal therapies are less-invasive treatments that destroy small prostate tumors without treating the rest of the prostate gland. These treatments use heat, cold, and other methods to treat cancer, mostly for low-risk or intermediate-risk prostate cancer. Focal therapies are being studied in clinical trials. Most have not been approved as standard treatment options.
Cryosurgery. Cryosurgery, also called cryotherapy or cryoablation, involves freezing cancer cells with a metal probe inserted through a small incision in the area between the rectum and the scrotum, the skin sac that contains the testicles. It is not an established therapy or standard of care to treat newly diagnosed prostate cancer. Cryosurgery has not been compared with radical prostatectomy or radiation therapy, so doctors do not know if it is a comparable treatment option. Its effects on urinary and sexual function are also not well known.
High-intensity focused ultrasound (HIFU). HIFU is a heat-based type of focal therapy. During HIFU treatment, an ultrasound probe is inserted into the rectum and then sound waves are directed at parts of the prostate gland with cancer. This treatment is designed to destroy cancer cells while limiting damage to the rest of the prostate gland. The FDA approved HIFU for the treatment of prostate tissue in 2015. HIFU may be an attractive option for some people, but knowing who may benefit most from this treatment is still unknown. HIFU should only be performed by a specialist with a lot of expertise. You will need to carefully discuss with your doctor if HIFU is the best treatment for you.
Return to top
Systemic treatments
The treatment plan may include medications to destroy cancer cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy.
This treatment is generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication.
Medications are often given through an intravenous (IV) tube placed into a vein using a needle or as a pill or capsule that is swallowed (orally). If you are given oral medications, be sure to ask your health care team about how to safely store and handle them.
The types of medications used for prostate cancer include:
-
Androgen-deprivation therapy (hormonal therapy)
-
Targeted therapy
-
Chemotherapy
-
Immunotherapy
-
Radiation therapy by infusion
-
Bone-modifying drugs
Each of these types of therapies is discussed below in more detail. A person may receive 1 type of medication at a time or a combination of medications given at the same time. They can also be given as part of a treatment plan that includes surgery and/or radiation therapy.
The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications.
It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases .
Androgen-deprivation therapy (hormonal therapy)
Because prostate cancer growth is driven by male sex hormones called androgens, lowering levels of these hormones can help slow the growth of the cancer. The most common androgen is testosterone. Androgen-deprivation therapy (ADT), or hormonal therapy, is used to lower testosterone levels in the body, either by surgically removing the testicles, known as surgical castration, or by taking drugs that turn off the function of the testicles, called medical castration. Which hormonal therapy is used is less important than the main goal of lowering testosterone levels.
Another way to stop testosterone from driving the growth of prostate cancer is to treat it with a type of medication called an androgen axis inhibitor. These medications can stop the body from making testosterone or stop testosterone from working. Androgen axis inhibitors include androgen receptor inhibitors and androgen synthesis inhibitors, which are both described in more detail below.
ADT is used to treat prostate cancer in many different situations, including localized, locally advanced, and metastatic prostate cancer, as well as rising PSA level after surgery and/or radiation therapy for localized prostate cancer. Some of the situations in which this therapy may be used include:
-
People with NCCN-based intermediate-risk and high-risk, localized prostate cancer who are having definitive therapy with radiation therapy are candidates for ADT. Definitive therapy is a treatment given with the intent to cure the cancer. People with intermediate-risk prostate cancer should receive ADT for at least 4 to 6 months. Those with high-risk prostate cancer should receive it for 2 to 3 years.
-
ADT may also be given to those who have had surgery and microscopic cancer cells were found in the removed lymph nodes. It is done to eliminate any remaining cancer cells and reduce the chance the cancer will return. This is known as adjuvant therapy. Although the use of adjuvant ADT is controversial, some specific patients appear to benefit from this approach.
Learn more about the basics of hormonal therapy .
Types of hormonal therapy for prostate cancer
Bilateral orchiectomy. Bilateral orchiectomy is the surgical removal of both testicles. It was the first treatment used for metastatic prostate cancer more than 70 years ago. Even though this is a surgical procedure, it is considered systemic hormonal therapy because it removes the main source of testosterone production: the testicles. The effects of this surgery are permanent and cannot be reversed. Bilateral orchiectomy is not commonly used anymore.
LHRH agonists. LHRH stands for luteinizing hormone-releasing hormone. Medications known as LHRH agonists prevent the testicles from receiving messages sent by the body to make testosterone. By blocking these signals, LHRH agonists reduce the testosterone level just as well as removing the testicles. Unlike orchiectomy, the effects of LHRH agonists are often reversible, so testosterone production usually begins again once treatment stops. However, testosterone recovery can take from 6 months to 24 months, and for a small number of patients, testosterone production does not return.
LHRH agonists are injected or placed as small implants under the skin. Depending on the drug used, they may be given once a month or once a year. When LHRH agonists are first given, testosterone levels briefly increase before falling to very low levels. This effect is known as a “flare.” Flares occur because the testicles temporarily release more testosterone in response to the way LHRH agonists work in the body. This flare may increase the activity of prostate cancer cells and cause symptoms and side effects, such as bone pain if the cancer has spread to the bone.
GnRH antagonist. GnRH stands for gonadotropin-releasing hormone. This class of drugs stops the testicles from producing testosterone like LHRH agonists, but they reduce testosterone levels more quickly and do not cause the flare associated with LHRH agonists. The U.S. Food and Drug Administration (FDA) has approved degarelix (Firmagon), given by monthly injection, to treat advanced prostate cancer. One side effect of this drug is that it may cause a severe allergic reaction. An oral GnRH antagonist, relugolix (Orgovyx), is also approved by the FDA for the treatment of advanced prostate cancer. Relugolix has a lower risk of causing serious heart problems in patients with preexisting heart disease. In addition, when treatment with relugolix is stopped, testosterone production is restored within weeks, rather than months, which may be helpful for those undergoing intermittent ADT (see below).
Androgen receptor (AR) inhibitors. While LHRH agonists and GnRH antagonists lower testosterone levels in the blood, androgen receptor (AR) inhibitors block testosterone from binding to so-called “androgen receptors,” which are chemical structures in cancer cells that allow testosterone and other male hormones to enter the cells. In effect, AR inhibitors stop testosterone from working. Newer AR inhibitors include apalutamide (Erleada), darolutamide (Nubeqa), and enzalutamide (Xtandi). Older AR inhibitors include bicalutamide (Casodex), flutamide (available as a generic drug), and nilutamide (Nilandron) and are taken as pills.
These medications are also sometimes called anti-androgens. AR inhibitors can be given to people who have “castration-sensitive” prostate cancer, which means that the prostate cancer still responds to treatments that lower testosterone levels. AR inhibitors are not usually used by themselves to treat prostate cancer.
-
Apalutamide. Apalutamide is approved by the FDA for the treatment of non-metastatic castration-resistant prostate cancer and for metastatic castration-sensitive prostate cancer in combination with ADT.
-
Darolutamide. Darolutamide is approved for the treatment of non-metastatic castration-resistant prostate cancer. It may also be used in combination with docetaxel chemotherapy to treat metastatic castration-sensitive prostate cancer.
-
Enzalutamide ( updated 11/2023 ). Enzalutamide is a nonsteroidal AR inhibitor that is approved to treat metastatic and non-metastatic castration-resistant prostate cancer as well as metastatic and non-metastatic castration-sensitive prostate cancer.
Androgen synthesis inhibitors. Although the testicles produce most of the body's testosterone, other cells in the body can still make small amounts of the hormone that may drive cancer growth. These include the adrenal glands and some prostate cancer cells. Androgen synthesis inhibitors target an enzyme called CYP17 and stop cells from making testosterone.
-
Abiraterone acetate (Zytiga). Abiraterone acetate is taken in the form of a pill. Patients may take abiraterone with prednisone (multiple brand names) or prednisolone (multiple brand names). Prednisone or prednisolone helps prevent some of the side effects of abiraterone.
-
Ketoconazole (Nizoral). Ketoconazole is an androgen synthesis inhibitor that is no longer widely used because of multiple drug interactions. However, ketoconazole may be an option for some patients.
Combined androgen blockade. Sometimes androgen receptor inhibitors are combined with bilateral orchiectomy or LHRH agonist treatment to maximize the blockade of male hormones or to prevent the flare associated with treatment with LHRH agonists (see above).
Intermittent ADT. Traditionally, ADT was given for the patient’s lifetime. During the past 2 decades, researchers have studied the use of intermittent ADT, which is when therapy is given for specific times (most commonly 6 months) and then stopped temporarily to allow for testosterone levels to recover. For these patients, ADT is restarted when the PSA begins to rise again. When to restart therapy (that is, at which PSA levels) is still a topic of debate. Using ADT in this way may lower the side effects related to the lack of testosterone and improve a person’s quality of life. ASCO recommends this approach only for people with high-risk PSA recurrence (see below) and with no evidence of metastatic disease after radical prostatectomy and/or radiation therapy. However, intermittent ADT has not been studied with chemotherapy or newer hormonal treatments, such as abiraterone or enzalutamide, so ASCO cannot recommend intermittent ADT with them.
Side effects of hormonal therapy
These treatments will cause side effects that generally go away after treatment has finished, except in those who have had an orchiectomy. General side effects include:
-
Erectile dysfunction
-
Loss of sexual desire
-
Hot flashes with sweating
-
Gynecomastia, which is growth of breast tissue that sometimes can lead to discomfort
-
Depression
-
Cognitive dysfunction and memory loss
-
Heart problems and heart disease
-
Weight gain
-
Loss of muscle mass
-
Osteopenia or osteoporosis, which is thinning of bones
Learn more about coping with the sexual side effects of prostate cancer treatment in the Coping With Treatment section.
Although testosterone levels may recover after stopping treatment, some who have received LHRH agonists for many years may continue to have hormonal effects, even if they are no longer taking these drugs.
Another serious side effect of these treatments is the risk of developing metabolic syndrome. Metabolic syndrome is a set of conditions, such as obesity, high levels of blood cholesterol, and high blood pressure, that increases a person’s risk of heart disease, stroke, and diabetes. Currently, it is not certain how often this happens or exactly why it happens, but it is quite clear that patients who receive ADT have an increased risk of developing metabolic syndrome. The risk is increased even if temporary medical castration is used. Find out more about the symptoms of hormone deprivation and how to manage them.
The risks and benefits of treatment should be carefully discussed with your doctor. For people with metastatic prostate cancer, especially if it is advanced and causing symptoms, most doctors believe that the benefits far outweigh the risks of side effects. It is highly encouraged that people receiving ADT take steps that help manage or avoid possible side effects. These include getting regular exercise, quitting smoking, eating a balanced diet, making sure to get enough vitamin D and calcium, and receiving comprehensive, preventive cardiovascular follow-up care.
Return to top
Targeted therapy
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. This type of treatment blocks the growth and spread of cancer cells and limits damage to healthy cells.
Not all tumors have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, research studies continue to find out more about specific molecular targets and new treatments directed at them. Learn more about the basics of targeted treatments .
Targeted therapy for prostate cancer includes:
-
Olaparib (Lynparza) ( updated 06/2023 ). Olaparib is a type of targeted therapy called a PARP inhibitor. It is approved for patients with metastatic castration-resistant prostate cancer whose disease has continued to grow and spread during treatment with abiraterone and/or enzalutamide and who have DNA-repair gene defects, which may be inherited or in the tumor. DNA-repair gene defects make it harder for cancer cells to repair damaged DNA. Certain genes, such as BRCA1 , BRCA2 , and several others, are linked with DNA-repair gene defects, and the presence of any of these can allow treatment with olaparib. Olaparib may be combined with abiraterone when used to treat new-onset metastatic castration-resistant prostate cancer with a BRCA mutation.
-
Rucaparib (Rubraca). Rucaparib is another PARP inhibitor approved to treat metastatic castration-resistant prostate cancer in patients whose disease has not been stopped by treatment with abiraterone and/or enzalutamide and chemotherapy, and who have a BRCA1 or BRCA2 mutation that is either inherited or in the tumor.
-
Talazoparib (Talzenna) ( updated 07/2023 ). Talazoparib is also a PARP inhibitor. It prevents cancer cells from repairing DNA damage by targeting a pathway called homologous recombination repair or HRR. Talazoparib is combined with enzalutamide to treat metastatic castration-resistant prostate cancer, but the cancer cells must have a mutation in the HRR gene.
-
Niraparib plus abiraterone (Akeega) ( updated 08/2023 ). Niraparib is a PARP inhibitor. When it is combined with abiraterone, it may be used to treat metastatic castration-resistant prostate cancer with a BRCA mutation.
One or more tests must be given to determine whether a patient may receive niraparib plus abiraterone, olaparib, or rucaparib:
-
Testing for an inherited, or germline, mutation after discussion with a genetic counselor
-
Genomic sequencing of tumor tissue
-
Genomic sequencing of the tumor DNA floating in the bloodstream
Genomic sequencing may be performed on tissue that was previously collected or on tissue from a new biopsy. Germline mutation testing alone identifies about half of the patients eligible for this treatment. People with metastatic prostate cancer who are considering targeted therapy are encouraged to talk with their doctors about all 3 tests mentioned above.
Talk with your doctor about possible side effects for a specific medication and how they can be managed.
Return to top
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells.
Chemotherapy may help those with advanced or castration-resistant prostate cancer and those with newly diagnosed or castration-sensitive metastatic prostate cancer. A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time.
There are several standard drugs used for prostate cancer. In general, standard chemotherapy begins with docetaxel (Taxotere) combined with prednisone.
Recent research shows adding docetaxel to ADT in those with newly diagnosed or castration-sensitive metastatic prostate cancer significantly helps people live longer and stops the disease from growing and spreading.
Cabazitaxel (Jevtana) is approved to treat metastatic castration-resistant prostate cancer that has been previously treated with docetaxel. It is a type of chemotherapy called a microtubule inhibitor.
The side effects of chemotherapy depend on the individual, the type of chemotherapy received, the dose used, and the length of treatment, but they can include fatigue, sores in the mouth and throat, diarrhea, nausea and vomiting, constipation, blood disorders, nervous system effects, changes in thinking and memory, sexual and reproductive issues, appetite loss, pain, and hair loss. The side effects of chemotherapy usually go away after treatment has finished. However, some side effects may continue, come back, or develop later. Ask your doctor which side effects you may experience, based on your treatment plan. Your health care team will work with you to manage or prevent many of these side effects.
Learn more about the basics of chemotherapy .
Return to top
Immunotherapy
Immunotherapy uses the body's natural defenses to fight cancer by improving your immune system’s ability to attack cancer cells.
For some people with castration-resistant metastatic prostate cancer who have no or very few cancer symptoms and generally have not had chemotherapy, vaccine therapy with sipuleucel-T (Provenge) may be an option.
Sipuleucel-T is adapted for each patient. Before treatment, blood is removed from the patient in a process called leukapheresis. Special immune cells are separated from the patient’s blood, modified in the laboratory, and then put back into the patient. At this point, the patient’s immune system may recognize and destroy prostate cancer cells. When this treatment is used, it is difficult to know if the treatment is working to treat the cancer because treatment with sipuleucel-T does not lead to lower PSA levels, shrinking of the tumor, or keeping the cancer from getting worse. However, results from clinical trials have shown that treatment with sipuleucel-T can lengthen lives by about 4 months in people with metastatic castration-resistant prostate cancer with few or no symptoms.
Different types of immunotherapy can cause different side effects. Common side effects include skin reactions, flu-like symptoms, diarrhea, and weight changes. Talk with your doctor about possible side effects for the immunotherapy recommended for you. Learn more about the basics of
immunotherapy
.
Return to top
Radiation therapy by infusion
Radium-223 (Xofigo). This treatment is a radioactive substance used to treat castration-resistant prostate cancer that has spread to the bone. Radium-223 is an alpha-emitter radionucleotide that mimics calcium and targets areas in the bone where the cancer is causing changes. This treatment delivers radiation particles directly to tumors found in the bone, limiting damage to healthy tissue, including the bone marrow, where normal blood cells are made. Radium-223 is given by intravenous injection (IV) once a month for 6 months. This treatment is given by a radiation oncologist or a nuclear medicine doctor. Your medical oncologist should continue to follow your progress during this treatment to make sure the treatment is helping and that any potential side effects are managed. Treatment with radium-233 does not dependably lower PSA, so patients should not expect to see big decreases in PSA levels during treatment and, in fact, often PSA levels may rise.
Some people should not receive this treatment, especially those who have prostate cancer that has spread to the liver and/or lungs and/or those with enlarged lymph nodes (3 cm or more in diameter). Radium-223 should not be used in combination with abiraterone and prednisone because that combination increases the risk of bone fractures. Discuss with your doctor whether this medication is an option for you.
Lutetium Lu 177 vipivotide tetraxetan (Pluvicto). This treatment, also called 177Lu-PSMA-617, targets a specific protein called PSMA (prostate-specific membrane antigen) that is highly expressed on prostate cancer cells, and it therefore delivers radiation directly to the cancer cells. It is approved for the treatment of people with metastatic castration-resistant prostate cancer who have already received an AR inhibitor and taxane chemotherapy, such as docetaxel. To receive this treatment, a special type of positron-emission tomography (PET) scan needs to confirm that the cancer cells express PSMA (see Diagnosis ). The most common side effects of this treatment include fatigue, dry mouth, nausea, anemia, loss of appetite, and constipation.
Return to top
Bone-modifying drugs
Bone health is an important issue in the lives of people with prostate cancer. Osteopenia and osteoporosis are bone conditions that can be caused or worsened by hormonal therapy. Patients receiving ADT for non-metastatic prostate cancer should be evaluated for risk of fractures. The most common way to find a person’s risk is with a dual-energy X-ray absorptiometry (DEXA) scan to measure the strength of the bones. Patients who are found to be at high risk for a fracture should receive treatment to lower the risk. Bone-modifying drugs that can be used in this situation include denosumab (Prolia, Xgeva), zoledronic acid (Reclast, Zometa), alendronate (Fosamax), risedronate (Actonel), ibandronate (Boniva), and pamidronate (Aredia). These medications can have side effects, so talk with your doctor about when to take the medication and which would be best based on your situation.
Bone-modifying drugs have not been shown to prevent the spread of prostate cancer to the bone in patients who do not currently have evidence of bone metastases.
In patients with prostate cancer that has spread to the bone, there is always some risk of bone problems, such as fracture, pain, and spinal cord compression. These are called “skeletal-related events.” When prostate cancer has spread to bone and has also become resistant to ADT (see "Metastatic castration-resistant prostate cancer" below), bone-modifying drugs may be recommended to reduce the risk of these problems. Specifically, denosumab or zoledronic acid can be given once per month to reduce that risk.
A rare but serious possible side effect of bone-modifying drugs is osteonecrosis of the jaw. The symptoms of osteonecrosis of the jaw include pain, swelling, and infection of the jaw; loose teeth; and exposed bone. The most prominent risk factor for this side effect is the need for invasive dental work (for example, tooth extraction) in a person who is already receiving a potent bone-modifying drug such as denosumab or zoledronic acid. It is important to have a dental evaluation before starting these drugs in order to assess safety and address problem areas before starting a bone-modifying drug. If someone taking these drugs needs dental work, treatment should be stopped until the dental work is completed and the patient has healed. Learn more about dental health and cancer.
This information is based on an ASCO endorsement of the Cancer Care Ontario guideline, “ Bone Health and Bone-targeted Therapies for Prostate Cancer .” Note that this link takes you to a different ASCO website.
Return to top
Physical, emotional, and social effects of cancer
Cancer and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Palliative care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after a cancer diagnosis. People who receive palliative care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments similar to those meant to get rid of the cancer, such as chemotherapy, surgery, or radiation therapy.
Before treatment begins, talk with your doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative care options. Many patients also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative care in a separate section of this website.
Return to top
Treatment by stage of prostate cancer
Different treatments may be recommended for each stage of prostate cancer. The general options by stage are described below. For more detailed descriptions, see “How prostate cancer is treated,” above. Your doctor will work with you to develop a specific treatment plan based on your specific diagnosis and needs. Clinical trials may also be a treatment option for each stage.
Early-stage prostate cancer (stages I and II)
Early-stage prostate cancer usually grows very slowly and may take years to cause any symptoms or other health problems, if it ever does at all. As a result, active surveillance or watchful waiting may be recommended. Radiation therapy (external-beam or brachytherapy) or surgery may also be suggested, as well as treatment in clinical trials. For those with a higher Gleason score, the cancer may be faster growing, so radical prostatectomy and radiation therapy are often recommended. Your doctor will consider your age and general health before recommending a treatment plan.
ASCO, the American Urological Association, American Society of Radiation Oncology, and the Society of Urologic Oncology recommend that patients with high-risk early-stage prostate cancer that has not spread to other areas of the body should receive radical prostatectomy or radiation therapy with ADT as standard treatment options.
Return to top
Locally advanced prostate cancer (stage III)
Locally advanced prostate cancer may be treated with external-beam radiation therapy and concurrent ADT or with surgery alone. ASCO recommends that doctors consider ADT to stop testosterone production plus abiraterone and prednisolone when patients can receive this approach. If abiraterone is not an option, combined androgen blockade using an AR inhibitor may be recommended. Treatments may be given in different combinations to stop the cancer from growing and spreading. Active surveillance is also an option. For those who have not received previous local treatment, including surgery, and who are unwilling or unable to receive radiation therapy, early (immediate) ADT may be offered.
It is widely accepted that at least 24 months of ADT is needed to control the disease, but 18 months may also be enough. For those who have a radical prostatectomy, radiation therapy is given after the surgery. This is called adjuvant or salvage radiation therapy. It is a standard of care for prostate cancer with extraprostatic extension, which is when the tumor has spread to nearby areas outside the prostate gland. Those with a high risk of bone fractures may be given a bone-modifying drug on an osteoporosis treatment dose and schedule (see "Bone-modifying drugs” above).
Watchful waiting may be considered for older adults who are not expected to live for a long time and whose cancer is not causing symptoms or for those who have another, more serious illness.
Return to top
Advanced prostate cancer (stage IV)
If cancer spreads to another part in the body from where it started, doctors call it metastatic cancer. High-risk or locally advanced prostate cancers have a higher chance of becoming metastatic cancer. If prostate cancer has a high risk of becoming metastatic or is already metastatic, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan. Clinical trials might also be an option. Learn more about getting a second opinion before starting treatment, so you are comfortable with your chosen treatment plan.
For many people, a diagnosis of advanced cancer is very stressful and difficult. You and your family are encouraged to talk about how you feel with doctors, nurses, social workers, or other members of your health care team. It may also be helpful to talk with other patients, such as through a support group or other peer support program.
There is no cure for metastatic prostate cancer, but it is often treatable for quite some time. Many people outlive their prostate cancer, even those who have advanced disease. Often, the prostate cancer grows slowly, and there are now effective treatment options that extend life even further. In this way, it can be like living with a chronic disease like heart disease or diabetes, requiring ongoing treatment to minimize symptoms and maintain well-being.
Supportive, or palliative, care to help relieve symptoms and side effects is an important part of the care of advanced prostate cancer. Supportive care options include:
-
TURP to manage symptoms such as bleeding or urinary obstruction (see "Surgery").
-
Bone-modifying drugs may be used to strengthen bones, reduce the risk of bone fractures, and reduce the risk of skeletal-related events for prostate cancer that has spread to the bone (see "Bone-modifying drugs").
-
Intravenous radiation therapy with radium-223, strontium, and samarium can also help relieve bone pain (see "Radiation therapy").
-
Palliative radiation therapy to specific bone areas can also be used to reduce bone pain when medications do not help.
Researchers are using other methods to better understand metastatic prostate cancer and identify new treatment approaches. For example, the Metastatic Prostate Cancer Project allows people with metastatic prostate cancer to enroll themselves. Please note that the link above takes you to another, independent website.
Biochemical or PSA recurrence ( updated 11/2023 )
Many people treated with surgery or radiation therapy are cured. However, some will develop a biochemical recurrence (BCR). The main signs of BCR are rising PSA levels and no metastases in scans. This is why BCR is also called "PSA recurrence" or “rising PSA syndrome.” Whether someone has BCR depends on what the first treatment for prostate cancer was.
For those who received a radical prostatectomy, BCR is defined as a rising PSA level that reaches a value of 0.2 ng/mL or more. Radiation therapy may be a treatment option for certain patients with BCR after surgery. This treatment is called “salvage radiation therapy.” Several factors are considered when deciding who can be treated with salvage radiation therapy, including Gleason score, pathologic stage, how long it took for BCR to happen, PSA level after surgery, and changes in PSA over time, also known as “PSA doubling time.”
For people who received radiation therapy as the main treatment for prostate cancer, BCR is defined as a normal testosterone level and a PSA value more than 2.0 ng/mL plus the lowest PSA value reached after the treatment with radiation therapy (this is called “nadir PSA”). Treating BCR after radiation therapy is more difficult. Treatment options can include surgery, called “salvage radical prostatectomy,” or cryosurgery, called “salvage cryotherapy” (see “Focal therapies,” above). You are encouraged to discuss the treatment options with the health care team.
ADT may be recommended, especially if other local treatments are not possible. For individuals with a high risk of metastasis, treatment with enzalutamide may be an option, regardless of whether the cancer was treated with prostatectomy or radiation therapy. If ADT is going to be used alone to treat the BCR, intermittent ADT may be an option.
Metastatic castration-sensitive prostate cancer ( Updated 04/2023)
Prostate cancer that has spread to other parts of the body and still responds to treatment that suppresses testosterone is called metastatic castration-sensitive prostate cancer. The best treatment option depends on the patient's health and the extent of the cancer. It is important to talk with the health care team about the risks and benefits of each option. Some of the following treatment options can only be used to treat people who are newly diagnosed. Others can be used to treat those who have received previous treatments, including radical prostatectomy (surgery) or radiation therapy.
For people who have newly diagnosed metastatic prostate cancer and who will be receiving chemotherapy with docetaxel, treatment options include:
-
ADT plus docetaxel and darolutamide (triplet therapy). In people with newly diagnosed metastatic prostate cancer, who were starting docetaxel plus ADT, research has shown that adding darolutamide to the regimen helps people live longer. If a patient is starting treatment with docetaxel plus ADT, ASCO recommends adding darolutamide to the regimen. This only applies to those who are receiving docetaxel chemotherapy.
-
ADT plus docetaxel plus abiraterone with prednisone or prednisolone (triplet therapy). In people with high-volume, newly diagnosed metastatic prostate cancer who were starting docetaxel plus ADT, research has shown that adding abiraterone to the regimen helps people live longer. If a patient is starting treatment with docetaxel plus ADT, ASCO recommends adding abiraterone to the regimen. This only applies to those who are receiving docetaxel chemotherapy.
-
ADT plus docetaxel. This treatment is reserved for those who are newly diagnosed and able to receive chemotherapy but who are unable to receive abiraterone. Docetaxel with or without ADT is given by IV every 3 weeks for a total of 6 doses.
For people with newly diagnosed, high-risk prostate cancer who are not candidates for chemotherapy, ASCO recommends the following treatment:
-
ADT plus abiraterone with prednisone or prednisolone. This treatment is recommended for people with newly diagnosed, high-risk metastatic castration-sensitive prostate cancer.
For people with newly diagnosed metastatic prostate cancer, regardless of how much the disease has spread, and who are not starting docetaxel chemotherapy, ASCO recommends the following treatments:
-
ADT plus enzalutamide or ADT plus apalutamide. These 2 treatment options are recommended as options for patients with metastatic castration-sensitive prostate cancer. These options are available even if the patient has already been treated with surgery, radiation therapy, or ADT.
In addition to the above treatment options, treatment to relieve symptoms and side effects continues to be an important part of the overall treatment plan.
This information is based in part on the ASCO guideline, “ Initial Management of Noncastrate Advanced, Recurrent, or Metastatic Prostate Cancer .” Note that this link takes you to a different ASCO website.
A bone-modifying drug may be recommended to prevent bone fractures (see " Bone-modifying drugs ” above).
Non-metastatic castration-resistant prostate cancer
Prostate cancer that is no longer stopped by low testosterone levels (less than 50 ng/mL) is called “castration resistant.” Castration-resistant prostate cancer is defined by a rising PSA level and/or worsening symptoms and/or growing cancer verified by scans. If the cancer has not spread to other parts of the body, it is called “non-metastatic castration-resistant prostate cancer.”
ASCO recommends that treatment for non-metastatic castration-resistant prostate cancer should continue to focus on lowering testosterone levels. This may include a permanent treatment, such as orchiectomy, or it may include continuing treatment with medications that lower hormone levels, such as apalutamide, darolutamide, or enzalutamide.
For those who have not had chemotherapy, additional ADT may be an option if there is a high risk that the disease will spread. Talk with your doctor about your personal risk level.
PSA testing and/or imaging tests may be done regularly to see if the cancer has worsened or spread. If there is a low risk of developing metastatic disease, ASCO recommends PSA testing every 4 to 6 months. If there is a high risk of metastatic disease, ASCO recommends PSA testing every 3 months. Imaging tests, such as a bone scan, CT scan, or magnetic resonance imaging (MRI), may be done if there are symptoms or signs that the cancer is worsening.
Metastatic castration-resistant prostate cancer ( updated 07/2023 )
If the cancer is no longer stopped by low testosterone levels (less than 50 ng/mL) and has spread to other parts of the body, it is called “metastatic castration-resistant prostate cancer.” Castration-resistant prostate cancer is defined by a rising PSA level and/or worsening symptoms and/or growing cancer verified by scans. ASCO recommends PSA testing every 3 months for metastatic castration-resistant prostate cancer. Generally, imaging tests, such as CT scan and bone scan, are done to check the growth and spread of cancer and to see how well treatment is working.
Metastatic castration-resistant prostate cancer can be difficult to treat. ASCO recommends continuing treatment that lowers hormone levels for metastatic castration-resistant prostate cancer. ASCO has treatment recommendations for hormone therapy for advanced cancer and for systemic treatment of metastatic castration-resistant prostate cancer .
Treatment options for metastatic castration-resistant prostate cancer are listed below. Treatment in a clinical trial may also be an option.
-
AR inhibitors, such as abiraterone or enzalutamide
-
Targeted therapy with olaparib or rucaparib
-
AR inhibitor combined with a PARP inhibitor
-
Chemotherapy with docetaxel, especially if there is bone pain or other cancer-related symptoms
-
Chemotherapy with cabazitaxel if docetaxel stops working
-
Immunotherapy with sipuleucel-T
-
Radioligand therapy (targeted radiation therapy by infusion) using 177Lu-PSMA-617
-
Radium-223, a form of radiopharmaceutical therapy (non-targeted radiation therapy by infusion)
-
Bone-modifying drugs to treat cancer that has spread to the bone
Return to top
Remission and the chance of recurrence
A remission is when cancer cannot be detected in the body and there are no symptoms. This may also be called having “no evidence of disease” or NED.
A remission can be temporary or permanent. This uncertainty causes many people to worry that the cancer will come back. Although there are treatments to help prevent a recurrence, such as hormonal therapy and radiation therapy, it is important to talk with your doctor about the possibility of the cancer returning. There are tools your doctor can use, called nomograms, to estimate someone's risk of recurrence. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the cancer does return. Learn more about coping with the fear of recurrence .
In general, following surgery or radiation therapy, the PSA level in the blood usually drops. If the PSA level starts to rise again, it may be a sign that the cancer has come back. If the cancer returns after the original treatment, it is called recurrent cancer.
If a recurrence happens, a new cycle of testing will begin again to learn as much as possible about it, including where the recurrence is located. The cancer may come back in the prostate (called a local recurrence), in the tissues or lymph nodes near the prostate (a regional recurrence), or in another part of the body, such as the bones, lungs, or liver (a distant or metastatic recurrence). Sometimes the doctor cannot find a tumor even though the PSA level has increased. This is known as a PSA recurrence or biochemical recurrence (BCR).
After this testing is done, you and your doctor will talk about the treatment options. The choice of treatment plan is based on the type of recurrence and the treatment(s) you have already received and may include the treatments described above, such as radiation therapy, prostatectomy for people first treated with radiation therapy, or ADT. Your doctor may suggest clinical trials that are studying new ways to treat recurrent prostate cancer.
Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects. Palliative care usually includes pain medication, external-beam radiation therapy, brachytherapy with radium-223, strontium, or samarium, or other treatments to reduce bone pain.
People with recurrent cancer sometimes experience emotions such as disbelief or fear. You are encouraged to talk with your health care team about these feelings and ask about support services to help you cope. Learn more about dealing with cancer recurrence .
Return to top
If treatment does not work
Recovery from cancer is not always possible. If the cancer cannot be cured or controlled, the disease may be called advanced or terminal.
This diagnosis is stressful, and for some people, advanced cancer may be difficult to discuss. However, it is important to have open and honest conversations with your health care team to express your feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families and is there to help. Making sure a person is physically comfortable, free from pain, and emotionally supported is extremely important.
People who have advanced cancer and who are expected to live less than 6 months may want to consider hospice care. Hospice care is designed to provide the best possible quality of life for people who are near the end of life. You and your family are encouraged to talk with the health care team about hospice care options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment, including a hospital bed, can make staying at home a workable option for many families. Learn more about advanced cancer care planning .
After the death of a loved one, many people need support to help them cope with the loss. Learn more about grief and loss .
Return to top
The next section in this guide is About Clinical Trials . It offers more information about research studies that are focused on finding better ways to care for people with cancer. Use the menu to choose a different section to read in this guide.
Prostate Cancer - About Clinical Trials
ON THIS PAGE: You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for people with prostate cancer. To make scientific advances, doctors create research studies involving volunteers, called clinical trials. Every drug that is now approved by the U.S. Food and Drug Administration (FDA) was tested in clinical trials.
Clinical trials are used for all types and stages of prostate cancer. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment.
People who participate in clinical trials can be some of the first to get a treatment many years before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. People are encouraged to talk with their health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a long time after treatment. Talk with your doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating prostate cancer. Even if they do not benefit directly from the clinical trial, their participation may benefit future people with prostate cancer.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about health insurance coverage of clinical trials .
Sometimes people have concerns that, in a clinical trial, they may receive no treatment by being given a placebo or a “sugar pill.” When used, placebos are usually combined with standard treatment in most cancer clinical trials. Study participants will always be told when a placebo is used in a study. Find out more about placebos in cancer clinical trials .
Patient safety and informed consent
To join a clinical trial, people participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options, so that the person understands how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different from the risks of standard treatment.
-
Explain what will be required of each person in order to participate in the clinical trial, including the number of doctor visits, tests, the schedule of treatment, and the costs they may need to pay.
-
Describe the purposes of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. You will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time for personal or medical reasons. This may include that the new treatment is not working or there are serious side effects. Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if they choose to leave the clinical trials before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all types of cancer. For specific topics being studied for prostate cancer, learn more in the Latest Research section.
Cancer.Net offers more information about cancer clinical trials in other areas of the website, including a complete section on clinical trials and places to search for clinical trials for a specific type of cancer .
In addition, you can find a free video-based educational program about cancer clinical trials in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for prostate cancer. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about prostate cancer and how to treat it. Use the menu to see other pages.
Doctors are working to learn more about prostate cancer, ways to prevent it, how to best treat it, and how to provide the best care to people diagnosed with this disease. The following areas of research may include new options for patients through clinical trials. Always talk with your doctor about the best diagnostic and treatment options for you.
-
Finding causes of prostate cancer. Researchers continue to explore the link between nutrition and other lifestyle factors and the development of prostate cancer.
-
Early detection. Researchers are trying to develop a better prostate-specific antigen (PSA) test, either a more specific and precise test or a different test. With improved testing, more healthy people could be screened for prostate cancer, so more prostate cancers could be found and treated early.
-
Genomic tests. Genomics is the study of how genes behave. Genomic tests look at the genes in prostate cancer to help predict how quickly the cancer may grow and spread. The information from these tests can help the cancer care team make decisions about the treatment plan, such as whether active surveillance is an option for those with low-risk prostate cancer or by helping the health care team make a prognosis after surgery and choose the best adjuvant treatments. Some of the genomic tests available now include Decipher, Oncotype DX, ProstaVysion, and the Prolaris Test.
The National Comprehensive Cancer Network (NCCN) recently updated their guidelines to include details about genomic testing in prostate cancer. They recommend that people with metastatic castration-resistant prostate cancer receive testing for inherited and tumor mutations, which could help direct treatment.
Learn more about ASCO recommendations for genomic tests for prostate cancer in the Diagnosis section.
-
Advanced imaging scans. Research is ongoing to use different molecules in PET-CT scans (positron-emission tomography, computed tomography; see Diagnosis ) to gather important information about a prostate cancer diagnosis, such whether there is distant spread (metastasis).
-
Improved surgical techniques. Better techniques for nerve-sparing surgery can decrease the risk of urinary and sexual side effects for people who need a radical prostatectomy.
-
Shorter radiation therapy schedules. With better, more precise external-beam radiation therapy, researchers are exploring much shorter and more convenient treatment schedules. Instead of 40 treatments, researchers are evaluating using 28, 12, or 5 treatments instead.
-
Tests to evaluate the success of treatment. Research continues to evaluate biomarkers that are found in the blood. These biomarkers can help determine the effectiveness of a treatment and be used to better assess the cancer’s response to treatment. Blood tests measuring circulating tumor cells (CTCs) are 1 such test. CTCs are cells that have broken free from the tumor.
-
Improved therapy for advanced prostate cancer. Researchers are exploring different treatment options for advanced prostate cancer in clinical trials, including special targeted drugs, chemotherapy, hormonal therapy, immunotherapy, and combinations of different types of therapies.
-
Palliative care/supportive care. Clinical trials are underway to find better ways of reducing symptoms and side effects of current prostate cancer treatments to improve comfort and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in prostate cancer, explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your doctor or search online clinical trial databases .
-
Visit the Cancer.Net Blog to review research in prostate cancer, including the 2022 Genitourinary Cancers Symposium and 2021 ASCO Annual Meeting , and to listen to podcasts with experts in the field discussing recent research.
-
Visit the website of Conquer Cancer, the ASCO Foundation , to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance on how to cope with the physical, emotional, social, and financial changes that cancer and its treatment can bring. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Coping with Treatment
ON THIS PAGE: You will learn more about coping with the physical, emotional, social, and financial effects of cancer and its treatment. Use the menu to see other pages.
Every cancer treatment can cause side effects or changes to your body and how you feel. For many reasons, people do not experience the same side effects even when they are given the same treatment for the same type of cancer. This can make it hard to predict how you will feel during treatment.
As you prepare to start cancer treatment, it is normal to fear treatment-related side effects . It may help to know that your health care team will work to prevent and relieve side effects. This part of cancer treatment is called palliative care or supportive care. It is an important part of your treatment plan, regardless of your age or the stage of disease.
Coping with physical side effects
Common physical side effects from each treatment option for prostate cancer are described in the Types of Treatment section. Learn more about side effects of cancer and its treatment, along with ways to prevent or control them . Changes to your physical health depend on several factors, including the cancer’s stage, the length and dose of treatment, and your general health. Any discussion of side effects should also cover fertility , sexual health and function , and problems with urination .
Talk with your health care team regularly about how you are feeling. It is important to let them know about any new side effects or changes in existing side effects. If they know how you are feeling, they can find ways to relieve or manage your side effects to help you feel more comfortable and potentially keep any side effects from worsening.
You may find it helpful to keep track of your side effects so it is easier to talk about any changes with your health care team. Learn more about why tracking side effects is helpful .
Sometimes, side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment are called late effects . Treating long-term side effects and late effects is an important part of survivorship care. Learn more by reading the Follow-up Care section of this guide or talking with your doctor.
Coping with sexual side effects
The treatment for prostate cancer can affect your sexual health. Some sexual side effects may be temporary and go away within a year after treatment, but some can be long lasting. Side effects that change sexual health can affect a person mentally, emotionally, and physically. Talk with your health care team about how your treatment will affect your sexual health. If you have a sexual partner, it can help to have an honest conversation with them about what worries you and what you expect may happen.
-
Loss of sexual desire. Treatments that reduce testosterone can lower your sexual desire. This will make you less interested in physical intimacy and having sex. It can also cause erectile dysfunction. There are no medical treatments to increase sexual desire, but treatments that lower testosterone may be temporarily stopped to let testosterone levels rise again. Fortunately, sexual desire is also influenced by other factors, such as relationship satisfaction, self-esteem, and psychological health. Because desire can be significantly dampened by loss of testosterone, it is important to learn how to optimize these other elements. Read a Cancer.Net Blog post about coping with the loss of sexual desire.
-
Erectile dysfunction. Erectile dysfunction or ED is when you cannot have or keep a penile erection. There are medications to help treat this condition, as well as medical devices like suppositories and a penile pump or implant. Read a Cancer.Net Blog post about asking for help with erectile problems.
-
Less semen and dry orgasm. Treatment may cause your orgasms to have less semen. Some treatments may result in orgasm with no semen at all. When this happens, it is called a dry orgasm. Having less or no semen does not affect a person’s feelings of pleasure during orgasm. However, it does affect your chances of fathering a child.
-
A smaller penis. Some patients may find that their penis shrinks by up to an inch after treatment, particularly after prostatectomy. Some research has found that this side effect is temporary, and the penis regains its size after a year. If this happens to you, speak with your health care team about penile rehabilitation, which can help with the recovery of the health of your penis.
There are many ways you can manage or cope with the sexual side effects of prostate cancer. The first step is to speak with your health care team about your sexual health, even if it makes you feel uncomfortable. Sexual recovery is an important part of quality of life, and your health care team can direct you to sources of help.
It will also be important to think about sexual arousal and intimacy in different ways. It may take longer to become aroused, you may feel distracted or anxious about cancer, and you may be uncomfortable talking with your partner about changes in your body image or erectile function. Often, it is helpful to focus on other forms of intimacy and sensual touch, such as kissing and cuddling, in order to enhance connection and jumpstart a sense of closeness and satisfaction. Most importantly, make time to communicate with your partner and seek help if you need it.
Cancer.Net has a page on sexual health for men , as well as a podcast about sexual health in people with prostate cancer and a general fact sheet that provides an overview of the sexual side effects of cancer.
Coping with emotional and social effects
You can have emotional and social effects after a cancer diagnosis. This may include dealing with a variety of emotions, such as sadness, anxiety, or anger, or managing your stress level. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about cancer.
You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your needs.
Coping with the costs of cancer care
Cancer treatment can be expensive. It may be a source of stress and anxiety for people with cancer and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their cancer treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Coping with barriers to care
Some groups of people experience different rates of new cancer cases and experience different outcomes from their cancer diagnosis. These differences are called “cancer disparities.” Disparities are caused in part by real-world barriers to quality medical care and social determinants of health , such as where a person lives and whether they have access to food and health care. Cancer disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , older adults , and people who live in rural areas or other underserved communities .
If you are having difficulty getting the care you need, talk with a member of your health care team or explore other resources that help support medically underserved people .
Talking with your health care team about side effects
Before starting treatment, talk with your doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should we call about side effects?
Be sure to tell your health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are serious. This discussion should include physical, emotional, social, and financial effects of cancer.
Caring for a loved one with cancer
Family members and friends often play an important role in taking care of a person with prostate cancer. This is called being a caregiver. Caregivers can provide physical, practical, and emotional support to the patient, even if they live far away. Being a caregiver can also be stressful and emotionally challenging. One of the most important tasks for caregivers is caring for themselves .
Caregivers may have a range of responsibilities on a daily or as-needed basis, including:
-
Providing support and encouragement
-
Talking with the health care team
-
Giving medications
-
Helping manage symptoms and side effects
-
Coordinating medical appointments
-
Providing a ride to and from appointments
-
Assisting with meals
-
Helping with household chores
-
Handling insurance and billing issues
A caregiving plan can help caregivers stay organized and help identify opportunities to delegate tasks to others. It may be helpful to ask the health care team how much care will be needed at home and with daily tasks during and after treatment. Use this 1-page fact sheet to help make a caregiving action plan. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of your symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Managing Pain: Get this 32-page booklet about the importance of pain relief that includes a pain tracking sheet to help patients record how pain affects them. The free booklet is available as a PDF, so it is easy to print out.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on anxiety and depression , diarrhea , rash , and immunotherapy side effects that provide a tracking sheet to record details about the side effect. These free fact sheets are available as a PDF, so they are easy to print, fill out, and give to your health care team.
The next section in this guide is Follow-up Care . It explains the importance of checkups after cancer treatment is finished. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Follow-Up Care
ON THIS PAGE: You will read about your medical care after cancer treatment is completed and why this follow-up care is important. Use the menu to see other pages.
Care for people diagnosed with prostate cancer does not end when active treatment has finished. Your health care team will continue to check that the cancer has not come back, manage any side effects, and monitor your overall health. This is called follow-up care.
Your follow-up care may include regular physical examinations, medical tests, or both. Doctors want to keep track of your recovery in the months and years ahead. Different people have different risks, so it is important to talk with your doctor about how your risk affects your schedule of follow-up care.
Cancer rehabilitation may be recommended, and this could mean any of a wide range of services, such as physical therapy, occupational therapy, career counseling, pain management, nutritional planning, and/or emotional counseling. The goal of rehabilitation is to help people regain control over many aspects of their lives and remain as independent as possible. Learn more about cancer rehabilitation.
Learn more about the importance of follow-up care .
Watching for recurrence
One goal of follow-up care is to check for a recurrence, which means that the cancer has come back. Cancer recurs because small areas of cancer cells may remain undetected in the body. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms. During follow-up care, a doctor familiar with your medical history can give you personalized information about your risk of recurrence. Your doctor will ask specific questions about your health. Some people may have blood tests or imaging tests done as part of regular follow-up care, but testing recommendations depend on several factors, including the type and stage of cancer first diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results may add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects
Most people expect to have side effects when receiving treatment. However, it is often surprising to survivors that some side effects may linger beyond the treatment period. These are called long-term side effects. Other side effects called late effects may develop months or even years after treatment has ended. Long-term and late effects can include both physical and emotional changes.
Talk with your doctor about your risk of developing late effects based on your diagnosis, your individual treatment plan, and your overall health. If you had a treatment known to cause specific late effects, you may have certain physical examinations, scans, or blood tests to help find and manage them.
Some common late effects of prostate cancer include:
-
Anemia , particularly for patients who have received or are receiving hormone therapy
-
Bowel problems, such as bleeding and needing to go to the bathroom urgently and/or frequently
-
Urinary problems , such as difficulty emptying the bladder or difficulty controlling the bladder, called incontinence
-
High blood pressure, high cholesterol, and blood sugar levels, particularly for patients who have received or are receiving hormone therapy
-
Depression
-
Anxiety
-
Bone problems , particularly for those who have received or are receiving hormonal therapy
-
Hot flashes , particularly for those who have received or are receiving hormonal therapy
-
Issues with sexual health, intimacy, and body image
Learn more about self-image and cancer , fertility and cancer treatment , sexual health , and talking with your spouse or partner .
General health recommendations
People recovering from prostate cancer are encouraged to follow established guidelines for good health, such as reaching and maintaining a healthy weight, exercising, not smoking, eating a balanced diet, and following cancer screening recommendations. Here are general recommendations for those recovering from prostate cancer:
-
Focus on eating more fruits, vegetables, and whole grains. Eat fewer high-calorie foods and beverages and less saturated fat.
-
Get at least 600 IU of vitamin D each day and no more than 1,200 milligrams of calcium per day from foods.
-
If you have problems that affect how well your body absorbs nutrients from foods, consider talking with a registered dietitian (RD).
-
Be physically active for at least 150 minutes each week.
-
Limit alcohol consumption to no more than 2 drinks per day.
-
Quit smoking or using other types of tobacco.
-
Follow recommendations for general cancer screening. Those who received radiation therapy for prostate cancer may have a higher risk of bladder and colorectal cancers and need more screening than usual.
Talk with your doctor or other member of your health care team to help you develop an exercise plan, eating plan, and cancer screening schedule that is best for you. In addition, if you smoke or use tobacco, talk with your health care team about resources to help you quit .
Keeping personal health records
You and your doctor should work together to develop a personalized follow-up care plan. Be sure to discuss any concerns you have about your future physical or emotional health. ASCO offers forms to help keep track of the cancer treatment you received and develop a survivorship care plan when treatment is completed.
This is also a good time to talk with your doctor about who will lead your follow-up care. Some survivors continue to see their oncologist, while others transition back to the care of their primary care doctor or another health care professional. This decision depends on several factors, including the type and stage of cancer, side effects, health insurance rules, and your personal preferences.
If a doctor who was not directly involved in your cancer care will lead your follow-up care, be sure to share your cancer treatment summary and survivorship care plan forms with them and with all future health care providers. Details about your cancer treatment are very valuable to the health care professionals who will care for you throughout your lifetime.
The next section in this guide is Survivorship . It describes how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Survivorship
ON THIS PAGE: You will read about how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to see other pages.
What is survivorship?
The word “survivorship” is complicated because it means different things to different people. Common definitions include:
-
Having no signs of cancer after finishing treatment.
-
Living with, through, and beyond cancer. According to this definition, cancer survivorship begins at diagnosis and continues during treatment and through the rest of a person's life.
For some, even the term “survivorship” does not feel right, and they prefer to use different language to describe and define their experience. Sometimes extended treatment will be used for months or years to manage or control cancer. Living with cancer indefinitely is not easy, and the health care team can help you manage the challenges that come with it . Everyone has to find their own path to name and navigate the changes and challenges that are the results of their cancer diagnosis and treatment.
Survivors may experience a mixture of feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after a cancer diagnosis and have gained a greater acceptance of themselves. Others become very anxious about their health and uncertain about coping with everyday life. Feelings of fear and anxiety may still occur as time passes, but these emotions should not be a constant part of your daily life. If they persist, be sure to talk with a member of your health care team.
Survivors may feel some stress when their frequent visits to the health care team end after completing treatment. Often, relationships built with the cancer care team provide a sense of security during treatment, and people miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, emotional challenges including fear of recurrence, sexual health and fertility concerns, and financial and workplace issues.
Every survivor has individual concerns and challenges. With any challenge, a good first step is being able to recognize your fears and talk about them. Effective coping requires:
-
Understanding the challenge you are facing
-
Thinking through solutions
-
Asking for and allowing the support of others
-
Feeling comfortable with the course of action you choose
Many survivors find it helpful to join an in-person support group or an online community of survivors. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of your health care team, individual counseling, or asking for assistance at the learning resource center of the place where you received treatment.
A new perspective on your health
For many people, survivorship serves as a strong motivator to make lifestyle changes.
People recovering from prostate cancer are encouraged to follow established guidelines for good health, such as not smoking, limiting alcohol, eating well, exercising regularly, maintaining a healthy weight, and managing stress. Regular physical activity can help rebuild your strength and energy level. Your health care team can help you create an appropriate exercise plan based upon your needs, physical abilities, and fitness level. Learn more about making healthy lifestyle choices .
It is important to have recommended medical checkups and tests (see Follow-up Care ) to take care of your health.
Talk with your health care team to develop a survivorship care plan that is best for your needs.
Changing role of caregivers
Family members and friends may also go through periods of transition. A caregiver plays a very important role in supporting a person diagnosed with cancer, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to the cancer diagnosis will become much less or come to an end. Caregivers can learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about cancer survivorship, explore these related items. Please note that these links will take you to other sections of Cancer.Net:
-
ASCO Answers Guide to Cancer Survivorship: Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. The free booklet is available as a PDF, so it is easy to print.
-
Survivorship Resources: Cancer.Net offers information and resources to help survivors cope, including specific sections for children , teens and young adults , and people over age 65 . There is also a main section on survivorship for people of all ages.
The next section offers Questions to Ask the Health Care Team to help start conversations with your cancer care team. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask your doctor or other members of the health care team to help you better understand your diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your health care. These suggested questions are a starting point to help you learn more about your cancer care and treatment. You are also encouraged to ask additional questions that are important to you. You may want to print this list and bring it to your next appointment, or download Cancer.Net’s free mobile app for an e-list and other interactive tools to manage your care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask about prostate cancer risk and screening
-
What type of prostate cancer screening schedule do you recommend for me, based on my individual medical profile and family history?
-
What are the risks and benefits of the prostate-specific antigen (PSA) test?
-
Are there any changes I can make to my diet that can help lower my risk of prostate cancer?
Questions to ask after getting a diagnosis
-
What type of prostate cancer do I have?
-
How aggressive is the cancer?
-
Can you explain my pathology report (laboratory test results) to me?
-
What stage is the prostate cancer? What does this mean?
-
What is the Gleason score of the prostate cancer? What does this mean?
Questions to ask about choosing a treatment and managing side effects
-
How much experience do you have treating this type of cancer?
-
What are my treatment options?
-
What clinical trials are available for me? Where are they located, and how do I find out more about them?
-
Does this prostate cancer need to be treated? What would happen if I choose not to start treatment now?
-
What treatment plan do you recommend? Why?
-
What is the goal of each treatment? Is it to eliminate the cancer, help me feel better, or both?
-
What are the possible side effects of each treatment, both in the short term and the long term?
-
How will treatment affect my emotional well-being?
-
Who will be part of my health care team, and what does each member do?
-
Who will be leading my overall treatment?
-
How will this treatment affect my daily life? Will I be able to work, exercise, and perform my usual activities?
-
Will I have difficulty controlling my bladder or bowel function after treatment?
-
Could this treatment affect my sex life? If so, how and for how long?
-
Could this treatment affect my ability to have children? If so, should I talk with a fertility specialist before cancer treatment begins? Should I consider sperm banking?
-
If I’m worried about managing the costs of cancer care, who can help me?
-
What support services are available to me? To my family?
-
If I have questions or problems, who should I call?
Questions to ask about having surgery
-
What type of surgery will I have? Will lymph nodes be removed?
-
How long will the operation take?
-
How long will I be in the hospital?
-
Can you describe what my recovery from surgery will be like?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term effects of having this surgery?
Questions to ask about having radiation therapy
-
What type of treatment is recommended?
-
Where will the radiation be focused?
-
What is the goal of this treatment?
-
How long will it take to give this treatment?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about having hormonal therapy
-
What type of hormonal therapy do you recommend?
-
What is the goal of this treatment?
-
How will this treatment be given?
-
Will I receive this treatment at a hospital or clinic? Or will I take it at home?
-
How long will I need to continue this treatment?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about having therapy using medication
-
What type of treatment do you recommend?
-
What is the goal of this treatment?
-
How will this treatment be given?
-
How long will it take to give this treatment?
-
Will I receive this treatment at a hospital or clinic? Or will I take it at home?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about planning follow-up care
-
What is the chance that the cancer will come back? Should I watch for specific signs or symptoms?
-
What long-term side effects or late effects are possible based on the cancer treatment I received?
-
What follow-up tests will I need, and how often will those tests be needed?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
Who will be leading my follow-up care?
-
What survivorship support services are available to me? To my family?
The next section in this guide is Additional Resources . It offers more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Prostate Cancer - Additional Resources
ON THIS PAGE: You will find some helpful links to other areas of Cancer.Net that provide information about cancer care and treatment. This is the final page of Cancer.Net’s Guide to Prostate Cancer. Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of cancer for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment, and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Search for a cancer specialist in your local area using this free database of doctors from the American Society of Clinical Oncology.
-
Learn what medical phrases and terms used in cancer care and treatment mean.
-
Read more about the first steps to take when you are diagnosed with cancer .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of cancer care.
-
Learn more about coping with the emotions that cancer can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for people with prostate cancer.
-
Explore what to do when you finish active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
-
Watch Cancer.Net videos with ASCO experts explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
-
For more information about treatment options for this disease, see the following topic review from UpToDate: Patient information: Prostate cancer treatment; stage I to III cancer (Beyond the Basics) . Please note that this link takes you to a separate, independent website.
-
The U.S. Centers for Disease Control and Prevention (CDC) has a virtual simulation called Talk to Nathan that can also help answer your questions about prostate cancer screening and treatment. (Please note that this link takes you to a different website.)
This is the end of Cancer.Net’s Guide to Prostate Cancer. Use the menu to choose a different section to read in this guide.