













Leukemia - Acute Myeloid - AML - Introduction
ON THIS PAGE: You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Adult Acute Myeloid Leukemia. Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
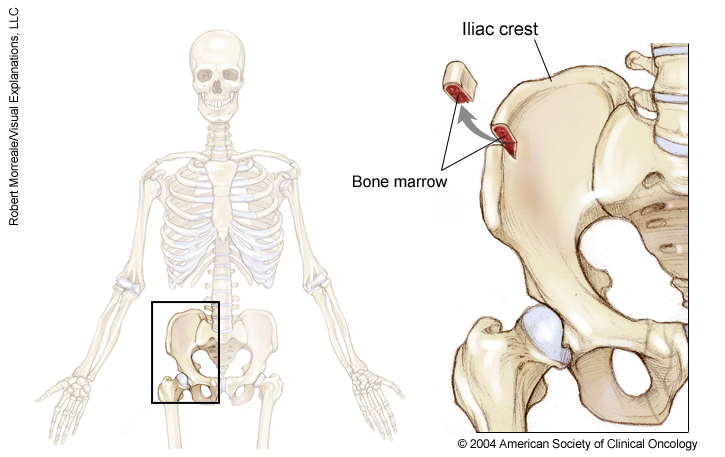
Leukemia is a cancer of the blood. It begins when healthy blood cells change and grow out of control. Acute myeloid leukemia (AML) starts in the bone marrow, the spongy tissue inside your bones that makes blood cells. AML may sometimes be called acute myelogenous leukemia, acute myelocytic leukemia, or acute nonlymphocytic leukemia.
Unlike chronic leukemia, acute leukemia develops quickly and generally needs immediate treatment. AML occurs in people of all ages but is most common in adults older than 65. This section is about AML in adults. Read about childhood AML in another section on this same website.
About bone marrow and blood cells
Bone marrow is the spongy, red tissue in the inner part of the large bones. It is where a person’s blood cells are made. Healthy immature blood cells are called myeloblasts or blasts . Blasts mature into one of 3 different types of blood cells:
-
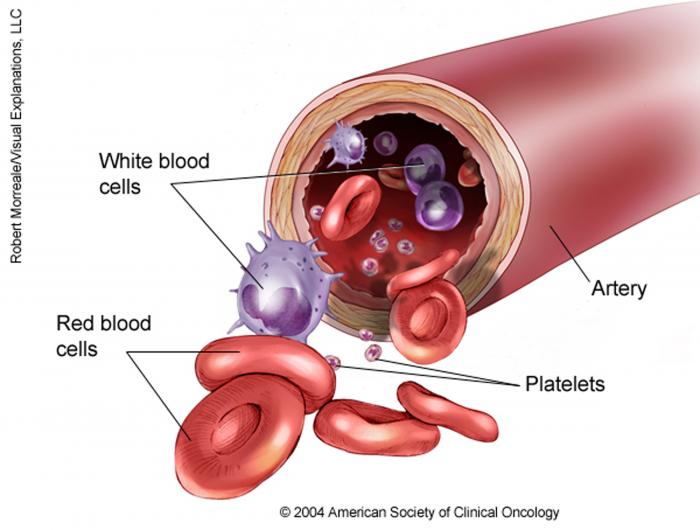
White blood cells, including neutrophils, which fight infection in the body
-
Red blood cells, which carry oxygen and other nutrients throughout the body
-
Platelets, which help the blood to clot
The bone marrow and blood cells are an important part of the body's immune system, which helps fight infection.
About AML
AML is caused by damage to the DNA in the bone marrow. This type of damage is called an acquired mutation. When the cells in the bone marrow are damaged, blood cells do not develop as they should. They may become abnormal, cancerous cells, which are also called blasts or myeloblasts because they look similar to healthy immature blast cells.
As they grow and divide, the cancerous myeloblasts fill up the bone marrow, preventing healthy cells from being made. They also build up in the blood stream. This reduces the number of healthy blood cells.
Therefore, people with AML are likely to have the following symptoms and signs :
-
Anemia, from not enough red blood cells, which can cause fatigue, weakness, and shortness of breath
-
Infections, because they do not have enough mature neutrophils
-
Easy bruising or bleeding, because of a low number of platelets
AML is usually found in the blood and bone marrow. It can sometimes spread to other parts of the body, such as the lymph nodes, spleen, liver, brain, skin, and gums. Occasionally, AML cells can form a solid tumor called a myeloid sarcoma or chloroma that can develop anywhere in the body. This is often called extramedullary disease.
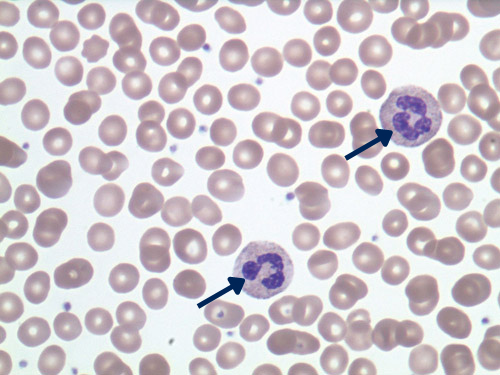
Normal peripheral blood with two neutrophils
Click to Enlarge
AML disease
Click to Enlarge
These images used with permission by the College of American Pathologists.
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to other sections on Cancer.Net:
- Cancer.Net En Español: Read about AML in Spanish . Infórmase sobre leucemia mieloide aguda .
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with AML and general survival rates. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Statistics
ON THIS PAGE: You will find information about the estimated number of people who will be diagnosed with acute myeloid leukemia (AML) each year. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with cancer are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this cancer and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for you individually. The original sources for these statistics are provided at the bottom of this page.
How many people are diagnosed with AML?
While leukemia in general is a common disease, the specific type of AML is uncommon, making up about 1% of cancers. In 2023, an estimated 20,380 people of all ages (11,410 men and boys and 8,970 women and girls) in the United States will be diagnosed with AML. The disease is the second most common type of leukemia diagnosed in adults and children, but most cases occur in adults. AML makes up 31% of all adult leukemia cases. Although AML can be diagnosed at any age, it is uncommon before age 45. The average age of diagnosis is age 68.
It is estimated that 11,310 deaths (6,440 men and boys and 4,870 women and girls) from this disease will occur in the United States in 2023. The majority will be among adults.
What is the survival rate for AML?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from AML. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having cancer may affect life expectancy. Relative survival rate looks at how likely people with AML are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this cancer.
Example: Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for people with AML are only an estimate. They cannot tell an individual person if cancer will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for people 20 and older with AML is 28%. For people younger than 20, the 5-year relative survival rate is 69%.
The survival rates for AML vary based on several factors. These include a person’s age and general health, and how well the treatment plan works. Another factor that can affect outcomes includes biologic features of the disease (see Subtypes for more information). Although AML is a serious disease, it is treatable and often curable with chemotherapy with or without a bone marrow/stem cell transplant (see the Types of Treatment section).
Experts measure relative survival rate statistics for AML every 5 years. This means the estimate may not reflect the results of advancements in how AML is diagnosed or treated from the last 5 years. Talk with your doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's (ACS) publication, Cancer Facts & Figures 2023, and the ACS website. (All sources accessed February 2023.)
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by AML. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Medical Illustrations
ON THIS PAGE: You will find drawings of the main body parts affected by acute myeloid leukemia (AML). Use the menu to see other pages.
The next section in this guide is Risk Factors . It describes the factors that may increase the chance of developing AML. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Risk Factors
ON THIS PAGE: You will find out more about the factors that increase the chance of developing acute myeloid leukemia (AML). Use the menu to see other pages.
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the development of cancer, most do not directly cause cancer. Some people with several risk factors never develop cancer, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
Although the cause of AML is not known, several factors are associated with an increased risk of the disease. The following factors may raise a person’s risk of developing AML:
-
Age. AML is more common in older adults, but it occurs at all ages. About half of people with AML are older than 65 when diagnosed.
-
Smoking. The risk of AML has been linked to exposure to tobacco smoke , probably along with other causes.
-
Genetic disorders. Increasingly, researchers are finding that leukemia may run in a family due to inherited gene mutations. AML occurs more often in people with the following inherited disorders:
-
Down syndrome
-
Ataxia telangiectasia
-
Li-Fraumeni syndrome
-
Klinefelter syndrome
-
Fanconi anemia
-
Wiskott-Aldrich syndrome
-
Bloom syndrome
-
Familial Platelet Disorder syndrome
-
Germline mutations which are present at birth, the most common of which are changes to the GATA2 , ETV6 , CEBPA , and RUNX1 genes
-
-
High doses of radiation. People who have been exposed to high levels of radiation may be more likely to develop AML. This includes people who have received radiation treatment for another cancer or long-term survivors of atomic bombs. Electromagnetic fields generated by high-voltage electrical power lines have not been shown to cause AML. Cell phone use is not a known risk factor for AML.
-
Chemotherapy. People who have received chemotherapy for another cancer may develop a therapy-related AML.
-
Chemicals. Long-term contact with products containing the chemical benzene, found in petroleum, cigarette smoke, and industrial workplaces, raises the risk of AML. However, exposure to industrial solvents and hair dyes has not been proven to increase a person’s risk of AML.
-
Other bone marrow disorders . People who have other bone marrow diseases including myeloproliferative disorders can develop AML over time. "Myelo-" means bone marrow and "proliferative" means too much. These conditions include:
-
Polycythemia vera
-
Myelofibrosis
-
Essential thrombocytosis
-
Myelodysplastic syndromes
-
Aplastic anemia
-
The next section in this guide is Symptoms and Signs . It explains what changes or medical problems AML can cause. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Symptoms and Signs
ON THIS PAGE: You will find out more about changes and other things that can signal a problem that may need medical care. Use the menu to see other pages.
People with acute myeloid leukemia (AML) may experience the following symptoms or signs. Symptoms are changes that you feel in your body. Signs are changes in something measured, like by taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem. Sometimes, people with AML do not have any of the signs and symptoms described below. Or, the cause of a symptom may be a medical condition that is not leukemia.
-
Fatigue
-
Weakness
-
Pale skin
-
Easy bruising or bleeding that does not stop easily
-
Weight loss
-
Fever
-
Bone, back, or abdominal pain
-
Difficulty breathing and/or shortness of breath
-
Frequent infections or infections that do not go away
-
Swollen lymph nodes or glands
-
Swollen or bleeding gums
-
Chest pain
-
Dizziness
-
Unusually long menstrual cycle
-
Skin nodules
-
Red, pin-head sizes spots on the skin
-
Wounds or sores that do not go away
-
Headache
-
Blurred vision
-
Soft tissue mass
If you are concerned about any changes you experience, please talk with your doctor. Your doctor will ask how long and how often you’ve been experiencing the symptom(s), in addition to other questions. This is to help figure out the cause of the problem, called a diagnosis .
If leukemia is diagnosed, relieving symptoms remains an important part of care and treatment. Managing symptoms may also be called "palliative care" or "supportive care." It is often started soon after diagnosis and continued throughout treatment. Be sure to talk with your health care team about the symptoms you experience, including any new symptoms or a change in symptoms.
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Diagnosis
ON THIS PAGE: You will find a list of the common tests, procedures, and scans that doctors can use to find out what’s wrong and identify the cause of the problem. Use the menu to see other pages.
How AML is diagnosed
There are many tests used for diagnosing AML. Doctors will also do tests to find out the subtype of AML (see Subtypes ). They may also do tests to learn which treatments could work best. Not all tests described here will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
-
The type of leukemia suspected
-
Your signs and symptoms
-
Your age and general health
-
The results of earlier medical tests
The following tests may be used to diagnose AML:
Blood tests.
To diagnose AML, a doctor will do
blood tests
to count the number of white blood cells and to see if they look abnormal under the microscope. Special lab tests called flow cytometry, or immunophenotyping, and cytochemistry are often used to distinguish AML from other types of leukemia and to determine the
exact subtype of AML
.
Bone marrow aspiration and biopsy.
These
2 procedures
are similar and often done at the same time to examine the bone marrow. Bone marrow has both a solid and a liquid part. A bone marrow aspiration removes a sample of the fluid with a needle. A bone marrow biopsy is the removal of a small amount of solid tissue using a needle.
A pathologist then analyzes the sample(s). A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease. A common site for a bone marrow aspiration and biopsy is the pelvic bone, which is located in the lower back by the hip. Doctors generally give a type of medication called anesthesia beforehand to numb the area. Stronger types of anesthesia can also be used to lessen the pain.
If blood tests (see above) indicate AML, it is better to have the bone marrow aspiration and biopsy at the hospital where the patient's cancer treatment will be given so the test does not need to be repeated.
Biomarker testing of the leukemia cells. Your doctor may recommend running laboratory tests to identify specific genes, proteins, and other factors involved in the leukemia. Examining the genes in the leukemia cells is very important because AML can be caused by a buildup of changes (also called mutations) in the cell’s genes. Identifying these changes helps diagnose the specific subtype of AML and choose treatment options. In addition, the results of those tests can also be used to monitor how well treatment is working. Listed below are the more common molecular or genetic tests used for AML.
-
Immunohistochemistry. This test uses a special dye to learn more about leukemia cells and find out the exact subtype of AML. The dye stains cells differently based on the kinds of chemicals in the cells, allowing doctors to determine the type of leukemia cells.
-
Flow cytometry. This test is also called immunophenotyping. Doctors use flow cytometry to measure different characteristics of cancer cells. AML cells have distinctive markers called surface markers. This test distinguishes AML cells from healthy blood cells and from other types of leukemia by identifying these markers.
-
Karotyping or cytogenetics. A karotype is a picture of a person's chromosomes. Chromosomes are found in the nuclei of cells within the body. Chromosomes are long strands of genes made up of DNA. Genes control how cells work by making proteins that have different functions. People usually have 23 pairs of chromosomes. Sometimes, people with cancer have certain changes to their chromosomes. Typically these changes develop during the person's lifetime and were not present at birth.
One type of change is called a translocation, which happens when a chromosome breaks off and reattaches to another chromosome. Knowing if there are certain translocations can help doctors determine the AML subtype and plan the best treatment. Flourescence-in-situ-hybridization (FISH) is a way to detect chromosome changes in cancer cells and is being used more often to help diagnose and determine the subtype of leukemia. This test is done on tissue removed during a biopsy or aspiration (see above).
Other types of chromosomal changes that can be present in some subtypes of leukemia include deletions and trisomies. Deletion is when part of a chromosome is missing. Trisomy is when there are extra copies of chromosomes.
Molecular testing. New testing methods have been developed to determine whether there are changes in the leukemia cells that may be helpful to understand how well treatment may work and whether targeted treatments may be an option (see the Types of Treatment section). There are many different types of molecular tests. It is common in AML for the doctor to order a panel of molecular tests that look at dozens of different genes that may be changed in leukemia cells.
Imaging tests. The imaging tests listed below may be used to learn more about the cause of symptoms or to help diagnose infections in patients with AML. They are not regularly used to find out how widespread the AML is because the disease has often spread throughout the bone marrow when it is first diagnosed.
-
Computed tomography (CT or CAT) scan. A CT scan is a test that creates pictures of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed, 3-dimensional image that shows any abnormalities. Sometimes, a special dye called a contrast medium is given before the scan to provide better detail on the image. This dye can be injected into a patient’s vein or given as a pill or liquid to swallow.
-
Magnetic resonance imaging (MRI). An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. A special dye called a contrast medium is given before these scans to create a clearer picture. This dye can be injected into a patient’s vein or given as a pill or liquid to swallow.
-
Positron emission tomography (PET) or PET-CT scan. A PET scan is usually combined with a CT scan (see above), called a PET-CT scan . However, you may hear your doctor refer to this procedure just as a PET scan. A PET scan is a way to create pictures of organs and tissues inside the body. A small amount of a radioactive sugar substance is injected into the patient’s body. This sugar substance is taken up by cells that use the most energy. Because cancer tends to use energy actively, it absorbs more of the radioactive substance. However, the amount of radiation in the substance is too low to be harmful. A scanner then detects this substance to produce images of the inside of the body. A PET scan may be used to find a myeloid sarcoma (see Introduction ) and find out how well treatment is working against the sarcoma.
Lumbar puncture, also called a spinal tap. A lumbar puncture is a procedure in which a needle is used to take a sample of cerebral spinal fluid (CSF) to look at the make up of the fluid and to find out if it contains leukemia cells or blood. CSF is the fluid that flows around the brain and spinal cord. Doctors generally give an anesthetic to numb the lower back before the procedure. The CSF is then examined under the microscope to look for AML cells. This is not a common test for AML.
After diagnostic tests are done, your doctor will review the results with you. If the diagnosis is AML, these results also help the doctor describe the disease. This is called subtyping.
The next section in this guide is Subtypes . It explains the way that doctors describe AML. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Subtypes
ON THIS PAGE: You will learn about how doctors describe AML. This is called the subtype. Use the menu to see other pages.
There are different ways to classify the subtypes of AML. Although all subtypes cause decreases in normal blood cell levels, different types of AML are associated with specific symptoms and problems. In addition, each subtype can behave differently after treatment.
Morphology
AML is first described by its morphology, or what the cancerous cells look like under the microscope. AML is classified by the type of normal, immature white blood cell it most closely resembles.
Most people with AML have a subtype called myeloid leukemia, which means the cancer is in the cells that normally produce neutrophils. Other patients have a type of AML called monoblastic or monocytic leukemia. In monocytic leukemia, the cells look like white blood cells called monocytes. Leukemia cells can also be a mixture of myeloblastic and monocytic cells.
Sometimes AML seems to come from cells that produce red blood cells, called erythroid cells, or platelets, called megakaryocytic cells.
Acute promyelocytic leukemia (APL) is a unique subtype of AML where the cancer cell stops maturing when the cell is at a stage called the promyelocyte or progranulocyte stage. APL is associated with a translocation between chromosomes 15 and 17 [t(15;17)].
The classification system from the World Health Organization (WHO) includes these major groups:
-
AML with recurrent genetic abnormalities, meaning with specific chromosomal or mutational changes
-
AML with myelodysplasia-related changes, or changes related to myelodysplastic syndromes (MDS)
-
AML with therapy-related myeloid neoplasms, which is damage caused by previous chemotherapy or radiation therapy
-
AML that is not otherwise categorized or NOS (not otherwise specified)
-
Myeloid sarcoma
-
Myeloid proliferations related to Down Syndrome
The French-American-British (FAB) classification is an older system for describing AML, but it may be used and is listed below for reference.
-
M0: Myeloblastic without differentiation
-
M1: Myeloblastic with little or no maturation
-
M2: Myeloblastic with maturation
-
M3: Promyelocytic
-
M4: Myelomonocytic
-
M4eo: Myelomonocytic with eosinophils
-
M5a: Monocytic without differentiation (monoblastic)
-
M5b: Monocytic with differentiation
-
M6: Erythroleukemic
-
M7: Megakaryocytic
Cytogenetics
AML is also classified by the cytogenetic, or chromosome, changes found in the leukemia cells. Certain chromosomal changes are closely matched with the morphology of the AML cells. More importantly, the chromosomal changes help doctors determine the best treatment options because these changes can sometimes predict how well intensive treatment will work. Chromosomal changes are commonly grouped according to the likelihood that treatment will work against the subtype of AML.
All chromosomes are numbered from 1 to 22. And, sex chromosomes are called “X” or “Y.” The letters “p” and “q” refer to the “arms” or specific areas of the chromosome. Some of the types of genetic changes found in AML include:
-
A translocation, which means that a chromosome breaks off and reattaches to another chromosome
-
Extra copies of a chromosome
-
A deletion of a chromosome
Some of the most common chromosomal changes are grouped as follows:
-
Favorable. Chromosomal changes associated with more successful treatment include abnormalities of chromosome 16 at bands p13 and q22 [t(16;16)(p13;q22), inv(16)(p13q22)] and a translocation between chromosomes 8 and 21 [t(8;21)].
-
Intermediate. Changes associated with a less favorable prognosis include normal chromosomes, where no changes are found and a translocation between chromosomes 9 and 11 [t(9;11)]. Many other subtypes are considered part of this group, particularly those with 1 or more specific molecular changes. Sometimes, extra copies of chromosome 8 or trisomy 8 may be classified as intermediate risk over unfavorable (see below).
-
Unfavorable. Examples of chromosomal changes that are associated with less successful treatment or with a low chance of curing the AML include extra copies of chromosomes 8 or 13 [for example, trisomy 8 (+8)], deletion of all or part of chromosomes 5 or 7, complex changes on many chromosomes, and changes to chromosome 3 at band q26.
Molecular Changes
Testing for molecular changes at diagnosis are very important to understand prognosis and treatment options along with chromosomal changes. Molecular genetic changes linked to prognosis for people with AML include:
-
NPM1
-
CEBP alpha
-
FLT3
-
RUNX1
-
ASXL1
-
TP53
-
IDH1 and IDH2
Patients with changes in the NPM1 or two mutated CEBP alpha genes have a better long-term outcome, while chemotherapy (see the Types of Treatment section) may work less for patients with changes in the FLT3, RUNX1, ASXL1 and TP53 mutations.
In general, the favorable changes occur more commonly in younger patients, while the unfavorable changes are more common in people older than 60. How well treatment works still varies widely in each of these groups. Treatment is successful in the long term for 50% to 60% of patients younger than 60 with AML that is classified as favorable and for less than 10% of patients younger than 60 with AML that is classified as unfavorable. Prognosis in patients older than 60 years of age is significantly worse. How well treatment works also depends on other factors, including the number of white blood cells. It is not possible to predict exactly the likelihood of successful treatment for a person with AML.
Recurrent AML
Recurrent or relapsed AML is cancer that has come back after treatment. If the AML does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis .
Information about the subtype will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment . Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Types of Treatment
ON THIS PAGE: You will learn about the different types of treatments doctors use for adults with acute myeloid leukemia (AML). Use the menu to see other pages.
This section explains the types of treatments, also known as therapies, that are the standard of care for AML. “Standard of care” means the best treatments known. When making treatment plan decisions, you are encouraged to discuss with your doctor whether clinical trials are an option. A clinical trial is a research study that tests a new approach to treatment. Doctors learn through clinical trials whether a new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option for all stages of leukemia. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
How AML is treated
In cancer care, different types of doctors often work together to create a patient’s overall treatment plan that combines different types of treatments. This is called a multidisciplinary team . Cancer care teams include a variety of other health care professionals, such as physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, dietitians, and others.
Treatment options and recommendations depend on several factors, including the subtype, morphology, and cytogenetics of AML (see Subtypes ), possible side effects, and the patient’s preferences and overall health.
Take time to learn about all of your treatment options and be sure to ask questions about things that are unclear. Talk with your doctor about the goals of each treatment and what you can expect while receiving the treatment. The goals of your care will drive your doctor's recommendations and where you seek treatment. If possible, it is helpful to have your treatment at a center experienced with treating AML. These types of talks are called “shared decision-making.” Shared decision-making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision-making is particularly important for AML because there are different treatment options. Learn more about making treatment decisions .
The common types of treatments used for AML are described below. Your care plan may also include treatment for symptoms and side effects, an important part of cancer care.
-
Intensive chemotherapy
-
Chemotherapy by phase
-
Side effects of chemotherapy
-
Targeted therapy
-
Acute promyelocytic leukemia (APL) treatment
-
Radiation therapy
-
Physical, emotional, and social effects of leukemia
-
Refractory AML
-
Remission and the chance of recurrence
-
If treatment does not work
Therapies using medication
Treatments using medication are used to destroy cancer cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy. Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body.
This treatment is generally prescribed by a medical oncologist or a hematologist. A medical oncologist is a doctor who specializes in treating cancer with medication. A hematologist is a doctor who specializes in treating blood disorders. Sometimes, a doctor can be trained as a medical oncologist and a hematologist. Both medical oncologists and hematologists may treat AML.
Medications to treat AML are given in different ways:
-
An intravenous (IV) tube placed into a vein using a needle. When chemotherapy is given by IV, it may be given into a larger vein or a smaller vein, such as in the arm. When it is given into a larger vein, a central venous catheter or port may need to be placed in the body.
-
An injection into the cerebral spinal fluid. This is called intrathecal therapy.
-
In a pill or capsule that is swallowed (orally)
-
An injection under the skin, called a subcutaneous injection
If you are given oral medications, be sure to ask your health care team about how to safely store and handle them.
The types of medications used for AML include:
-
Chemotherapy
-
Targeted therapy
Each of these types of therapies are discussed below in more detail. A person may receive 1 type of medication at a time or a combination of medications given at the same time. They can also be given as part of a treatment plan that includes other treatments.
The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications.
It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases .
Intensive chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells. Chemotherapy is the primary treatment for AML.
A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A patient may receive 1 drug at a time or a combination of different drugs given at the same time. Several drugs are used to treat AML, which are discussed below.
Learn more about the basics of chemotherapy .
Return to top
Chemotherapy by phase
Chemotherapy for AML can be divided into 3 phases: induction, post-remission consolidation, and maintenance.
Induction therapy.
This is the first period of treatment after a person’s diagnosis. The goal of induction therapy is a complete remission (CR). A person has a CR when:
-
Blood counts have returned to normal
-
Leukemia cannot be found in a bone marrow sample when examined under the microscope
-
There are no longer any signs and symptoms of AML
The combination of cytarabine (Cytosar-U) given over 4 to 7 days and an anthracycline drug, such as daunorubicin (Cerubidine) or idarubicin (Idamycin), given for 3 days is used most often. Targeted therapy (see below) may also be a recommended part of this treatment.
Patients may also be given hydoxyurea (Droxia, Hydrea) to help lower white blood cell counts before starting induction therapy. In addition to killing leukemia cells, these drugs also damage healthy cells, increasing the risk of infection and bleeding (see below). Most patients will need to stay in the hospital for 3 to 5 weeks during induction therapy before their blood counts return to normal. Sometimes, 2 rounds of therapy are needed to achieve a CR. Approximately 75% of younger adults with AML and about 50% of patients older than 60 achieve a CR after treatment.
Some older adults may not be able to have induction therapy with the standard drugs. The drugs of azacitidine (Vidaza), low-dose cytarabine, decitabine (Dacogen), glasdegib (Daurismo), and venetoclax (Venclexta, Venclyxto) may be used instead. A clinical trial is also an option.
Post-remission Consolidation. After induction therapy, a variety of different drugs are used to destroy AML cells that remain in small amounts that cannot be detected by medical tests. AML will almost certainly recur if no further treatment is given after a CR. For some patients, bone marrow/stem cell transplantation (see below) is recommended as part of post-remission therapy.
Chemotherapy or stem cell transplantation may be used for consolidation therapy.
-
Younger adults in remission are commonly given 2 to 4 rounds of high- or intermediate-dose cytarabine or other intensive chemotherapy at monthly intervals. Several different regimens are used for older patients. Although chemotherapy is usually given in the hospital, most of the recovery time can be spent at home.
-
A bone marrow/stem cell transplantation is often recommended as post-remission consolidation therapy for patients in whom cytogenetic or molecular studies predict a poorer prognosis with only chemotherapy or targeted therapy.
Maintenance. Even after completion of post-remission consolidation, there is a risk that AML can still return. Lower strength medications can be given on an ongoing basis for several years to reduce the chance of the disease returning, called recurrence. Medications such as azacitidine (Vidaza), decitabine (Dacogen), or midostaurin (Rydapt) are examples.
Bone marrow transplantation/stem cell transplantation.
A bone marrow transplant is a medical procedure in which bone marrow that contains leukemia is destroyed and then replaced by highly specialized cells. These cells, called hematopoietic stem cells, develop into healthy bone marrow. Hematopoietic stem cells are blood-forming cells found both in the bloodstream and in the bone marrow. This procedure is also called a stem cell transplant or hematopoietic stem cell transplant.
Before recommending transplantation, doctors will talk with the patient about the risks of this treatment. They will also consider several other factors, such as the type of leukemia, results of any previous treatment, and patient’s age and general health.
There are 2 types of hematopoietic stem cell transplantation depending on the source of the replacement blood stem cells: allogeneic (ALLO) and autologous (AUTO). ALLO uses donated stem cells, while AUTO uses the patient’s own stem cells. ALLO transplants are generally used for AML.
The goal is to destroy all of the cancer cells in the marrow, blood, and other parts of the body using high doses of chemotherapy and/or radiation therapy and then allow replacement blood stem cells to create healthy bone marrow.
Side effects depend on the type of transplant, your general health, and other factors. Learn more about the basics of
stem cell and bone marrow transplantation
.
Return to top
Side effects of chemotherapy
Chemotherapy for AML attacks rapidly dividing cells, including those in healthy tissues, such as the hair, lining of the mouth, intestines, and bone marrow. People with AML receiving chemotherapy may lose their hair , develop mouth sores , or have nausea and vomiting. Hair will regrow after treatment is finished, and there are effective drugs to help prevent and control nausea and vomiting . The side effects of chemotherapy may be different depending on the drugs used. Patients are encouraged to talk with their doctors about short-term and long-term side effects before treatment begins.
Because of the effect on healthy blood cells in the bone marrow, chemotherapy used for AML will lower the body’s ability to fight infection for a short time, and increased bruising, bleeding, and fatigue may be common. People with AML often receive antibiotics to prevent and treat infections and will need transfusions of red blood cells and platelets throughout chemotherapy. Chemotherapy may also affect the patient’s fertility , or ability to have a child in the future. Patients concerned about this are encouraged to talk with a fertility specialist before treatment begins.
Return to top
Targeted therapy
Targeted therapy is a treatment that targets the leukemia’s specific genes, proteins, or the tissue environment that contributes to the growth and survival of the leukemia. This type of treatment blocks the growth and spread of leukemia cells and limits damage to healthy cells.
Not all cancers have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, research studies continue to find out more about specific molecular targets and new treatments directed at them. Learn more about the basics of
targeted treatments
.
The following targeted treatments may be used for AML, depending on the gene mutations found in the leukemia cells:
Drugs targeting FLT3 gene mutations. There are 2 drugs approved to AML with an FLT3 gene mutation. About 25% to 30% of people with AML have AML with an FLT3 mutation.
-
Midostaurin (Rydapt) is approved in combination with chemotherapy to treat people who have been newly diagnosed with AML with an FLT3 mutation.
-
Gilteritinib (Xospata) is approved to treat relapsed or refractory AML with an FLT3 mutation.
Drugs targeting IDH1 or IDH2 gene mutations. There are 2 drugs and 1 drug combination approved to treat relapsed or refractory AML with IDH1 and IDH2 mutations. About 10% of people with AML have AML with an IDH1 or IDH2 mutation.
-
Enasidenib (IDHIFA) is approved to treat relapsed or refractory AML with an IDH2 mutation.
-
Ivosidenib (Tibsovo) is approved to treat relapsed or refractory AML with an IDH1 mutation.
-
Ivosidenib (Tibsovo) is also approved in combination with azacitidine (Vidaza), a type of chemotherapy, for newly diagnosed AML, with an IDH1 mutation, in patients aged 75 years and older or patients under 75 years of age with co-existing conditions preventing use of intensive induction chemotherapy.
Talk with your doctor about possible side effects for a specific medication and how they can be managed
Return to top
Acute promyelocytic leukemia (APL) treatment
The treatment of the APL subtype of AML is very different. This subtype is very sensitive to the effects of all-trans retinoic acid (ATRA). ATRA is a drug that is similar to vitamin A and is given by mouth. People with the APL subtype who receive a combination of ATRA and arsenic trioxide (Trisenox) are very likely to have a CR and be cured. Less commonly, chemotherapy containing regimens (see above) with idarubicin, daunorubicin, or cytarabine may also be used. Arsenic trioxide may be used during induction therapy alone or in combination with ATRA during post-remission therapy or if APL comes back after treatment.
Mild to severe bleeding is a common symptom of APL. Patients with this subtype often need many platelet and blood transfusions during initial treatment. Some patients with APL may benefit from use of ATRA plus low dose oral chemotherapy for 1 to 2 years after the initial treatment.
Return to top
Radiation therapy
Radiation therapy is the use of high-energy x-rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. The most common type of radiation therapy is called external-beam radiation therapy, which is radiation given from a machine outside the body. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time. Because AML is found throughout the blood, radiation therapy is generally used only when leukemia cells have spread to the brain or to shrink a myeloid sarcoma.
Side effects from radiation therapy may include fatigue, mild skin reactions, upset stomach, and loose bowel movements. Most side effects go away soon after treatment is finished. Learn more about the basics of radiation therapy .
Return to top
Physical, emotional, and social effects of leukemia
Leukemia and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the leukemia.
Palliative care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after diagnosis. People who receive palliative care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments similar to those meant to get rid of the leukemia, such as chemotherapy or radiation therapy.
Before treatment begins, talk with your doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative care options. Many patients also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative care in a separate section of this website.
Return to top
Refractory AML
If leukemia is still present after initial treatment, the disease is called refractory AML. If this happens, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan. Clinical trials might also be an option. Learn more about getting a second opinion before starting treatment, so you are comfortable with your chosen treatment plan.
Your treatment plan may include new drugs being tested in clinical trials. An ALLO bone marrow/stem cell transplant (see above) should also be considered. Palliative care will also be important to help relieve symptoms and side effects.
Return to top
Remission and the chance of recurrence
A remission is when the leukemia cannot be detected in the body, there are no symptoms, and a patient’s blood counts are normal. This may also be called having “no evidence of disease” or NED.
A remission may be temporary or permanent. This uncertainty causes many people to worry that the cancer will come back. While many remissions are permanent, it is important to talk with your doctor about the possibility of the leukemia returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the disease does return. Learn more about
coping with the fear of recurrence
.
If the leukemia returns after the original treatment, it is called recurrent or relapsed leukemia. If the leukemia returns, a new cycle of testing will begin again to learn as much as possible about the recurrence. After this testing is done, you and your doctor will talk about the treatment options. Often the treatment plan will include the treatments described above, such as chemotherapy, stem cell transplantation, targeted therapy, and radiation therapy, but they may be used in a different combination or given at a different pace. Your doctor may suggest clinical trials that are studying new ways to treat this type of recurrent leukemia. Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects.
The treatment for recurrent AML often depends on the length of the initial remission. If the AML comes back after a long remission, the original treatment may work again. If the remission was short, then other drugs are used, often through a clinical trial. An ALLO stem cell transplant may be the best option for patients whose leukemia has come back after initial treatment. However, many drugs and other approaches are being researched in clinical trials and these may provide other treatment options.
People with recurrent leukemia sometimes experience emotions such as disbelief or fear. You are encouraged to talk with your health care team about these feelings and ask about support services to help you cope. Learn more about
dealing with cancer recurrence
.
Return to top
If treatment does not work
Recovery from leukemia is not always possible. If the leukemia cannot be cured or controlled, the disease may be called advanced or terminal.
This diagnosis is stressful, and for some people, advanced leukemia may be difficult to discuss because it is incurable. However, it is important to have open and honest conversations with your health care team to express your feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families and is there to help. Making sure a person is physically comfortable, free from pain, and emotionally supported is extremely important.
People with advanced leukemia who have no more effective treatment options available may want to consider hospice care. Hospice care is designed to provide the best possible quality of life for people who are near the end of life. You and your family are encouraged to talk with the health care team about hospice care options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment can make staying at home a workable option for many families. Learn more about
advanced cancer care planning
.
After the death of a loved one, many people need support to help them cope with the loss. Learn more about
grief and loss
.
Return to top
The next section in this guide is About Clinical Trials . It offers more information about research studies that are focused on finding better ways to care for people with cancer. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - About Clinical Trials
ON THIS PAGE: You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for people with acute myeloid leukemia (AML). To make scientific advances, doctors create research studies involving volunteers, called clinical trials. Every drug that is now approved by the U.S. Food and Drug Administration (FDA) was tested in clinical trials.
Clinical trials are used for all types and stages of AML. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment. People who participate in clinical trials can be some of the first to get a treatment before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. People are encouraged to talk with their health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a lo ng time after treatment. Talk with your doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating AML. Even if they do not benefit directly from the clinical trial, their participation may benefit future people with AML.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about health insurance coverage of clinical trials .
Sometimes people have concerns that, in a clinical trial, they may receive no treatment by being given a placebo or a “sugar pill.” When used, placebos are usually combined with standard treatment in most cancer clinical trials. Study participants will always be told when a placebo is used in a study. Find out more about placebos in cancer clinical trials.
Patient safety and informed consent
To join a clinical trial, people must participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options, so that the person understands how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different from the risks of standard treatment.
-
Explain what will be required of each person in order to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.
-
Describe the purpose of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. You will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time for personal or medical reasons. This may include that the new treatment is not working or there are serious side effects. Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if they choose to leave the clinical trial before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all types of cancer. For specific topics being studied for AML, learn more in the Latest Research section.
Cancer.Net offers more information about cancer clinical trials in other areas of the website, including a complete section on clinical trials and places to search for clinical trials for a specific type of cancer .
In addition, you can find a free video-based educational program about cancer clinical trials located in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for AML. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about AML and how to treat it. Use the menu to see other pages.
Doctors are working to learn more about acute myeloid leukemia (AML), ways to prevent it, how to best treat it, and how to provide the best care to people diagnosed with this disease. The following areas of research may include new options for patients through clinical trials. Most cancer centers are actively involved in clinical trials focused on increasing the number of people cured of AML. Always talk with your doctor about the best diagnostic and treatment options for you.
-
Understanding AML biology. Research on the biology of AML is ongoing to learn more about how leukemia develops and to improve its treatment, particularly for older patients.
-
New drugs and treatment regimens. Researchers are looking at the use of existing drugs given in different doses and schedules, as well as new drugs. Specific research includes the use of drugs called hypomethylating therapy, such as azacitidine or decitabine. Targeted therapies and immunotherapy treatments are also being researched. Targeted therapies use drugs to target specific genes and proteins to treat cancer. Immunotherapy treatment boost the body's natural defenses to fight cancer.
-
Targeted therapy. Researchers are studying ways to block how specific genetic changes found in AML cells affect the body. Quizartinib and crenolanib are investigational drugs that stop the mutated FLT3 gene from working that are being tested in clinical trials. Other targeted therapies are being researched that stop AML cells from becoming resistant to chemotherapy when the chemotherapy stops working. Specific targeted therapy drugs being researched include venetoclax (Venclexta) and other drugs that are targeted to specific gene mutations such as IDH1 (ivositenib), c-KIT, and RAS .
-
Immunotherapy. Immunotherapy , also called biologic therapy, is designed to boost the body’s natural defenses to fight the leukemia. It uses materials made either by the body or in a laboratory to improve, target, or restore immune system function. Researchers are specifically looking at vaccines and the use of antibodies directed against the AML cells. Researchers are also looking at adoptive immunotherapy techniques. This type of immunotherapy involves changing a person’s white blood cells in a laboratory to increase their ability to fight the tumor. The changed cells are given back to the patient.
-
Stem cell/bone marrow transplantation. Different ways to make stem cell transplantation safer, easier, and more effective are also being studied (see Types of Treatment ).
-
Palliative care/supportive care . Clinical trials are underway to find better ways of reducing symptoms and side effects of current AML treatments to improve comfort and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in AML explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your doctor or search online clinical trial databases .
-
Listen to a podcast from an ASCO expert discussing highlights from the ASCO20 Virtual Scientific Program .
-
Visit the website of Conquer Cancer, the ASCO Foundation to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance in how to cope with the physical, emotional, social, and financial changes that AML and its treatment can bring. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Coping with Treatment
ON THIS PAGE : You will learn more about coping with the physical, emotional, social, and financial effects of cancer and its treatment. Use the menu to see other pages.
Every treatment for leukemia can cause side effects or changes to your body and how you feel. For many reasons, people do not experience the same side effects even when they are given the same treatment for the same type of leukemia. This can make it hard to predict how you will feel during treatment.
As you prepare to start treatment, it is normal to fear treatment-related side effects . It may help to know that your health care team will work to prevent and relieve side effects. This part of treatment is called palliative care or supportive care. It is an important part of your treatment plan, regardless of your age or the subtype of disease.
Coping with physical side effects
Common physical side effects from each treatment option for acute myeloid leukemia (AML) are described in the Types of Treatment section. Learn more about side effects of leukemia and its treatment, along with ways to prevent or control them . Changes to your physical health depend on several factors, including the leukemia’s subtype, the length and dose of treatment, and your general health.
Talk with your health care team regularly about how you are feeling. It is important to let them know about any new side effects or changes in existing side effects. If they know how you are feeling, they can find ways to relieve or manage your side effects to help you feel more comfortable and potentially keep any side effects from worsening.
You may find it helpful to keep track of your side effects so it is easier to talk about any changes with your health care team. Learn more about why tracking side effects is helpful .
Sometimes, side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment are called late effects . Treating long-term side effects and late effects is an important part of survivorship care. Learn more by reading the Follow-up Care section of this guide or talking with your doctor.
Coping with emotional and social effects
You can have emotional and social effects after an AML diagnosis. This may include dealing with a variety of emotions, such as sadness, anxiety, or anger, or managing your stress level. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about cancer.
You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your needs.
Coping with the costs of cancer care
Treatment can be expensive. It may be a source of stress and anxiety for people with AML and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Coping with barriers to care
Some groups of people experience different rates of new cancer cases and experience different outcomes from their cancer diagnosis. These differences are called "cancer disparities." Disparities are caused in part by real-world barriers to quality medical care and social determinants of health , such as where a person lives and whether they have access to food and health care. Cancer disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , older adults , and people who live in rural areas or other underserved communities .
If you are having difficulty getting the care you need, talk with a member of your health care team or explore other resources that help support medically underserved people .
Talking with your health care team about side effects
Before starting treatment, talk with your doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should we call about side effects?
Be sure to tell your health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are serious. This discussion should include physical, emotional, social, and financial effects of AML.
Caring for a loved one with AML
Family members and friends often play an important role in taking care of a person with AML. This is called being a caregiver. Caregivers can provide physical, practical, and emotional support to the patient, even if they live far away. Being a caregiver can also be stressful and emotionally challenging. One of the most important tasks for caregivers is
caring for themselves
.
Caregivers may have a range of responsibilities on a daily or as-needed basis, including:
-
Providing support and encouragement
-
Talking with the health care team
-
Giving medications
-
Helping manage symptoms and side effects
-
Coordinating medical appointments
-
Providing a ride to and from appointments
-
Assisting with meals
-
Helping with household chores
-
Handling insurance and billing issues
A caregiving plan can help caregivers try to stay organized and help identify opportunities to delegate tasks to others. It may be helpful to ask the health care team how much care will be needed at home and with daily tasks during and after treatment. Use this 1-page fact sheet to help make a caregiving action plan. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of your symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Managing Pain: Get this 32-page booklet about the importance of pain relief that includes a pain tracking sheet to help patients record how pain affects them. The free booklet is available as a PDF, so it is easy to print.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on anxiety and depression , constipation , diarrhea , and rash that provide a tracking sheet to record the details about the side effect. These free fact sheets are available as a PDF, so they are easy to print, fill out, and give to your health care team.
The next section in this guide is Follow-up Care and it explains the importance of checkups after treatment for AML is finished. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Follow-Up Care
ON THIS PAGE: You will read about your medical care after treatment is completed and why this follow-up care is important. Use the menu to see other pages.
Care for people diagnosed with acute myeloid leukemia (AML) does not end when active treatment has finished. Your health care team will continue to check that the leukemia has not come back, manage any side effects, and monitor your overall health. This is called follow-up care.
Your follow-up care may include regular physical examinations, medical tests, or both. Doctors want to keep track of your recovery in the months and years ahead. Cancer rehabilitation may be recommended, and this could mean any of a wide range of services, such as physical therapy, occupational therapy, career counseling, pain management, nutritional planning, and/or emotional counseling. The goal of rehabilitation is to help people regain control over many aspects of their lives and remain as independent as possible.
Learn more about cancer rehabilitation
.
Learn more about the importance of follow-up care .
Watching for recurrence
One goal of follow-up care is to check for a recurrence, which means that the leukemia has come back. Leukemia recurs because small areas of leukemia cells may remain undetected in the body. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms. During follow-up care, a doctor familiar with your medical history can give you personalized information about your risk of recurrence. Your doctor will ask specific questions about your health. Some people may have blood tests or imaging tests done as part of regular follow-up care, but testing recommendations depend on several factors, including the subtype of AML first diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results may add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects
Most people expect to have side effects when receiving treatment. However, it is often surprising to survivors that some side effects may linger beyond the treatment period. These are called long-term side effects. Other side effects called late effects may develop months or even years after treatment ends. Long-term and late effects can include both physical and emotional changes.
Talk with your doctor about your risk of developing such side effects based on the subtype of AML, your individual treatment plan, and your overall health. If you had a treatment known to cause specific late effects, you may have certain physical examinations, scans, or blood tests to help find and manage them.
Keeping personal health records
You and your doctor should work together to develop a personalized follow-up care plan. Be sure to discuss any concerns you have about your future physical or emotional health. ASCO offers forms to help keep track of the treatment you received and develop a survivorship care plan when treatment is completed.
This is also a good time to talk with your doctor about who will lead your follow-up care. Some survivors continue to see their oncologist, while others transition back to the care of their primary care doctor or another health care professional. This decision depends on several factors, including the subtype of AML, side effects, health insurance rules, and your personal preferences.
If a doctor who was not directly involved in your care for AML will lead your follow-up care, be sure to share your treatment summary and survivorship care plan forms with them, and with all future health care providers. Details about your treatment are very valuable to the health care professionals who will care for you throughout your lifetime.
The next section in this guide is Survivorship . It describes how to cope with challenges in everyday life after a diagnosis of AML. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Survivorship
ON THIS PAGE: You will read about how to cope with challenges in everyday life after a diagnosis of acute myeloid leukemia (AML). Use the menu to see other pages.
What is survivorship?
The word “survivorship” is complicated because it means different things to different people. Common definitions include:
-
Having no signs of cancer after finishing treatment.
-
Living with, through, and beyond cancer. According to this definition, cancer survivorship begins at diagnosis and continues during treatment and through the rest of a person's life.
For some, even the term "survivorship" does not feel right, and they prefer to use different language to describe and define their experience. Sometimes extended treatment will be used for months or years to manage or control cancer. Living with cancer indefinitely is not easy, and the health care team can help you manage the challenges that come with it . Everyone has to find their own path to name and navigate the changes and challenges that are the result of their cancer diagnosis and treatment.
Survivors may experience a mixture of feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after the diagnosis and have gained a greater acceptance of themselves. Others become very anxious about their health and uncertain about coping with everyday life. Feelings of fear and anxiety may still occur as time passes, but these emotions should not be a constant part of your daily life. If they persist, be sure to talk with a member of your health care team.
Survivors may feel some stress when their frequent visits to the health care team end after completing treatment. Often, relationships built with the health care team provide a sense of security during treatment, and people miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, emotional challenges including fear of recurrence, sexual health and fertility concerns, and financial and workplace issues.
Every survivor has individual concerns and challenges. With any challenge, a good first step is being able to recognize your fears and talk about them. Effective coping requires:
-
Understanding the challenge you are facing
-
Thinking through solutions
-
Asking for and allowing the support of others
-
Feeling comfortable with the course of action you choose
Many survivors find it helpful to join an in-person support group or an online community of survivors. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of your health care team, individual counseling, or asking for assistance at the learning resource center of the place where you received treatment.
A new perspective on your health
For many people, survivorship serves as a strong motivator to make lifestyle changes.
People recovering from AML are encouraged to follow established guidelines for good health, such as not smoking, limiting alcohol, eating well, exercising regularly, and managing stress. Regular physical activity can help rebuild your strength and energy level. Your health care team can help you create an appropriate exercise plan based upon your needs, physical abilities, and fitness level. Learn more about
making healthy lifestyle choices
.
It is important to have recommended medical checkups and tests (see
Follow-up Care
) to take care of your health.
Talk with your health care team to develop a survivorship care plan that is best for your needs.
Changing role of caregivers
Family members and friends may also go through periods of transition. A caregiver plays a very important role in supporting a person diagnosed with leukemia, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to the diagnosis will become much less or come to an end. Caregivers can learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about survivorship, explore these related items. Please note that these links will take you to other sections of Cancer.Net:
-
ASCO Answers Cancer Survivorship Guide : Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. This free booklet is available as a PDF, so it is easy to print.
-
Survivorship Resources : Cancer.Net offers information and resources to help survivors cope, including specific sections for children , teens and young adults , and people over age 65 . There is also a main section on survivorship for people of all ages.
The next section offers Questions to Ask the Health Care Team to help start conversations with your health care team. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask your doctor or other members of the health care team, to help you better understand your diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your health care. These suggested questions are a starting point to help you learn more about your care and treatment. You are also encouraged to ask additional questions that are important to you. You may want to print this list and bring it to your next appointment, or download Cancer.Net’s free mobile app for a digital list and other interactive tools to manage your care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask after getting a diagnosis
-
What is my diagnosis? What does it mean?
-
What subtype of acute myeloid leukemia (AML) do I have?
-
Do I need to start treatment right away?
-
Can you recommend a leukemia specialist?
-
Can you explain my pathology report (laboratory test results) to me?
Questions to ask about choosing a treatment and managing side effects
-
Where is the best place for me to receive treatment?
-
What are my options for treatment?
-
What clinical trials are available for me? Where are they located, and how do I find out more about them?
-
What treatment plan do you recommend? Why?
-
What is the goal of each treatment? Is it to eliminate the leukemia, manage the symptoms or side effects, or both?
-
How likely is it that my AML will go into remission? What does that mean?
-
Who will be part of my health care team, and what does each member do?
-
Who will be leading my overall treatment?
-
What are the possible side effects of this treatment, both in the short term and the long term?
-
Could this treatment affect my sex life? If so, how and for how long?
-
Could this treatment affect my ability to become pregnant or have children? If so, should I talk with a fertility specialist before treatment begins?
-
How will the treatment affect my daily life? Will I be able to work, exercise, and perform my usual activities?
-
If I’m worried about managing the costs of medical care, who can help me?
-
What support services are available to me? To my family?
-
If I have questions or problems, who should I call?
Questions to ask about having chemotherapy, targeted therapy, or a bone marrow/stem cell transplant
-
What type of treatment is recommended?
-
What is the goal of this treatment?
-
How long will it take to give this treatment?
-
Will I receive this treatment at a hospital or clinic? Or will I take it at home?
-
How long will treatment last overall?
-
Will I need to stay in the hospital during treatment? Why and when?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about planning follow-up care
-
What is the chance that the AML will come back? Should I watch for specific signs or symptoms?
-
What long-term side effects or late effects are possible based on the treatment I received?
-
What follow-up tests will I need, and how often will those tests be needed?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
Who will be leading my follow-up care?
-
What survivorship support services are available to me? To my family?
The next section in this guide is Additional Resources . It offers more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Myeloid - AML - Additional Resources
ON THIS PAGE: You will find some helpful links to other areas of Cancer.Net that provide information about care and treatment. This is the final page of Cancer.Net’s Guide to Acute Myeloid Leukemia in Adults. Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of leukemia for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment, and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Search for a specialist in your local area using this free database of doctors from the American Society of Clinical Oncology.
-
Learn what medical phrases and terms used in medical care and treatment mean .
-
Read more about the first steps to take when you are diagnosed with leukemia .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of medical care.
-
Learn more about coping with the emotions that leukemia can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for people with AML.
-
Explore what to do when you finish active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
-
Watch Cancer.Net videos with ASCO experts explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
-
For more information about treatment options for this disease, see UpToDate: Patient Information on AML (Beyond the Basics) . Please note that this link takes you to a separate, independent website.
This is the end of Cancer.Net’s Guide to Adult Acute Myeloid Leukemia. Use the menu to choose a different section to read in this guide.