













Leukemia - Acute Lymphoblastic - ALL - Childhood - Introduction
ON THIS PAGE:
You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Childhood Acute Lymphoblastic Leukemia (ALL). Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
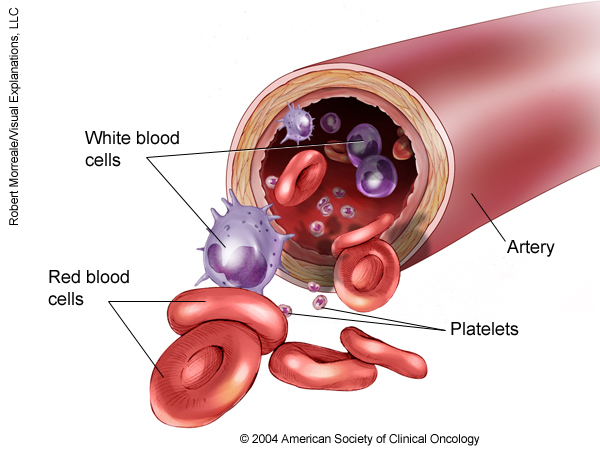
Leukemia is a cancer of the blood. Leukemia begins when healthy blood cells change and grow uncontrollably. Acute lymphoblastic leukemia (ALL) is a cancer of the lymphocytes, a type of white blood cell involved in the body’s immune system. ALL is the most common type of cancer in children.
About lymphocytes and lymphoblasts
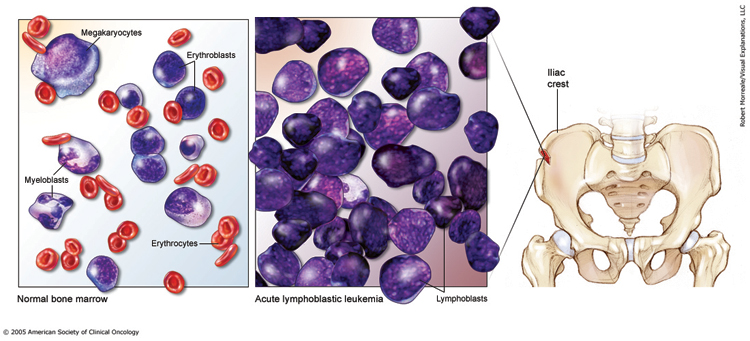
Lymphocytes are made in the bone marrow, the spongy, red tissue in the inner part of the large bones. Lymphocytes are found in the blood, lymph nodes, and spleen. Healthy lymphocytes fight bacterial and viral infections. In children with ALL, new lymphocytes do not develop into mature cells, but stay as immature cells called lymphoblasts.
About ALL
When a child has ALL, the lymphoblasts fill the bone marrow and crowd out other normal cells, preventing the production of red blood cells (cells that carry oxygen to tissues), many other types of normal white blood cells (cells that fight infection), and platelets (cells that help blood to clot). If the bone marrow is not functioning correctly, the child may experience anemia, easy bruising, bleeding, or infection.
-
Anemia is from too few red blood cells. Anemia can lead to fatigue, irritability, sleepiness, paleness, shortness of breath, and a rapid heartbeat.
-
Bruising or bleeding from injuries may occur more easily because the blood cannot clot normally when the platelet count is low.
-
Infection may occur more often if the blood has too few normal white blood cells. Many types of white blood cells are needed to fight infections caused by different germs.
The leukemic lymphoblasts may also collect in the child’s lymph nodes and cause them to swell. Lymphoblasts may also spread to other organs, including the skin, liver, spleen, the spinal fluid, ovaries, and testicles.
This section is about ALL in children, sometimes called childhood ALL or pediatric ALL. Learn more about acute lymphocytic leukemia in adults .
Looking for More of an Introduction?
If you would like additional introductory information, explore these related items. Please note these links will take you to other sections on Cancer.Net:
- Cancer.Net En Español : Read about childhood ALL in Spanish . Infórmase sobre la leucemia linfocítica aguda infantil en español .
The next section in this guide is Statistics . It helps explain the number of children who are diagnosed with childhood acute lymphoblastic leukemia (ALL) and general survival rates. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Statistics
ON THIS PAGE: You will find information about the estimated number of children and teens who will be diagnosed with acute lymphoblastic leukemia (ALL) each year, also called childhood ALL. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with cancer are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this cancer and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for your child individually. The original sources for these statistics are provided at the bottom of this page.
How many children and teens are diagnosed with ALL?
ALL is the most common type of childhood cancer. In the United States, approximately 75% of people under age 20 diagnosed with leukemia are diagnosed with ALL. Most cases occur between ages 2 and 5. However, it can be diagnosed at any age. An estimated 400 people ages 15 to 19 in the United States are diagnosed with the disease each year.
ALL is less common in girls than boys. Hispanic children and White children are slightly more likely to develop ALL than Asian children and Black children.
What is the survival rate for childhood ALL?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from ALL. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having cancer may affect life expectancy. Relative survival rate looks at how likely people with ALL are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this cancer.
Example: Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for children and teens with ALL are only an estimate. They cannot tell an individual person if cancer will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for children 0 to 14 with ALL is 92%. The 5-year relative survival rate for teens ages 15 to 19 is 77%. The survival rates for children and teens with ALL vary based on several factors. These include the classification of the age and general health, and how well the treatment plan works.
For younger patients diagnosed with acute leukemia, those who remain free from the disease after 5 years are generally considered cured because it is rare for acute leukemia to recur after this amount of time.
Experts measure relative survival rate statistics for childhood ALL every 5 years. This means the estimate may not reflect the results of advancements in how ALL is diagnosed or treated from the last 5 years. Talk with your child’s doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's (ACS) publications, Cancer Facts & Figures 2023 and Cancer Facts & Figures 2020: Special Section - Cancer in Adolescents and Young Adults, and the ACS website. (All sources accessed February 2023.)
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by childhood ALL. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Medical Illustrations
ON THIS PAGE: You will find drawings of the main body parts affected by this disease. Use the menu to see other pages.
The next section in this guide is Risk Factors . It describes what factors may increase the chance of developing childhood acute lymphoblastic leukemia (ALL). Use the menu to choose a different section to read this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Risk Factors
ON THIS PAGE : You will find out more about the factors that increase the chance of developing childhood acute lymphoblastic leukemia (ALL). Use the menu to see other pages.
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the development of cancer, most do not directly cause cancer. Some people with several risk factors never develop cancer, while others with no known risk factors do.
Although doctors don’t know what causes most childhood leukemia, some evidence shows that certain genetic factors play a role in ALL.
Children who are born with a condition that has been linked to genetic and immune system problems -- such as Down syndrome,
ataxia telangiectasia
, or Bloom syndrome -- may have a higher risk of developing leukemia.
A child with an identical twin that develops ALL before age 6 has an increased risk of developing leukemia. If an identical twin develops leukemia within the first few months of life, the other twin will almost always develop the same type of leukemia.
The next section in this guide is Symptoms and Signs . It explains what changes or medical problems that childhood ALL can cause. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Symptoms and Signs
ON THIS PAGE : You will find out more about changes and other things that can signal a problem that may need medical care. Use the menu to see other pages.
Children with acute lymphoblastic leukemia (ALL) may experience the following symptoms or signs. Symptoms are changes that you can feel in your body. Signs are changes in something measured, like by taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem. Sometimes, children with ALL do not have any of the symptoms and signs described below. Or, the cause of a symptom or sign may be a medical condition that is not cancer.
The early signs of ALL can look like the flu or other common illnesses. When 1 or more of these symptoms last for longer than you would expect, or you are worried about a symptom or sign on this list, please talk with your child's doctor.
-
Frequent infections
-
A fever that doesn’t go away
-
Feeling weak and tired all the time
-
Bone pain
-
Swollen lymph nodes (for example, in the neck, under the arms, or in the groin)
-
Paleness
-
Bruising or bleeding easily
-
Difficulty breathing
-
Headache
-
Enlarged liver or spleen
If you are concerned about any changes your child experiences, please talk with your child’s doctor. Your doctor will ask how long and how often your child has been experiencing the symptom(s), in addition to other questions. This is to help figure out the cause of the problem, which is called a diagnosis.
If ALL is diagnosed, relieving symptoms remains an important part of cancer care and treatment. Managing symptoms may also be called "palliative care" or "supportive care." It is often started soon after diagnosis and continued throughout treatment. Be sure to talk with your child’s health care team about the symptoms your child experiences, including any new symptoms or a change in symptoms.
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Diagnosis
ON THIS PAGE : You will find a list of the common tests, procedures, and scans that doctors can use to find the cause of a medical problem. Use the menu to see other pages.
Doctors use many tests to find, or diagnose, leukemia. They also do tests to learn if cancer has spread to another part of the body from where it started. If the cancer has spread, it is called metastasis. Doctors may also do tests to learn which treatments could work best.
How acute lymphoblastic leukemia (ALL) is diagnosed
There are many tests used for diagnosing ALL. Not all tests described here will be used for every person. Your child's doctor may consider these factors when choosing a diagnostic test:
-
The type of cancer suspected
-
Your child's signs and symptoms
-
Your child's age and general health
-
The results of earlier medical tests
A patient history, physical examination, complete blood cell count (CBC), and bone marrow aspiration (see below) are the main procedures used to diagnose ALL or rule out other conditions.
-
Blood tests. A CBC provides a count of each type of cell in the blood. The blood count may also show abnormal leukemia cells. The blood count is abnormal, in some way, for nearly all children with ALL when they are diagnosed. A blood chemistry test gives information about the body’s kidney and liver function, as well as other measures, such as salt levels.
-
Bone marrow aspiration and biopsy. These 2 procedures are similar and often done at the same time to examine the bone marrow. Bone marrow has both a solid and a liquid part. A bone marrow aspiration removes a sample of the fluid with a needle. A bone marrow biopsy is the removal of a small amount of solid tissue using a needle.
A pathologist then analyzes the sample(s). A common site for a bone marrow aspiration and biopsy is the pelvic bone, which is located in the lower back by the hip. Doctors generally give a type of medication called anesthesia beforehand to numb the area. Anesthesia is medication that blocks the awareness of pain. Stronger types of anesthesia can also be used to lessen the pain.
A bone marrow aspiration is recommended if the blood test shows unusual blood counts or immature cells, or if the doctor suspects that a child may have leukemia. From this test, the doctor can find out whether the child has leukemia and, if so, what type of leukemia it is. The doctor or other health care team member will collect more than one sample of bone marrow at the same time for other tests, such as chromosome and molecular genetic tests and immunophenotyping (see Classification ). These additional tests are important to plan the most appropriate treatments.
-
Lumbar puncture (spinal tap). A lumbar puncture can determine if the leukemia has spread to the cerebral spinal fluid (CSF). CSF is the fluid that flows around the brain and the spinal cord. During a lumbar puncture, a needle is used to take a sample of the CSF to look for leukemia cells. Doctors may give an anesthetic to numb the lower back before the procedure and/or use anesthesia to block awareness of the pain. Knowing whether or not there is leukemia in the central nervous system helps doctors choose the most appropriate treatment. All children with ALL receive medicine to treat or prevent leukemia of the central nervous system at the same time as the lumbar puncture at specific times during treatment.
After diagnostic tests are done, your child’s doctor will review the results with you. If the diagnosis is ALL, these results also help the doctor describe the disease. This is called classification .
The next section in this guide is Classification. It explains the system doctors use to describe this type of cancer. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Classification
ON THIS PAGE: You will learn about the factors that doctors use to describe this type of cancer. This is called classification. Use the menu on the side of your screen.
There is no staging system for childhood acute lymphoblastic leukemia (ALL), unlike some other types of cancer. However, there are a number of factors that help doctors choose the best treatment plan and predict the chance that the disease will come back after treatment. Doctors plan each child’s treatment based on these and other factors:
-
Age. Infants younger than 12 months and children age 10 and older need more intensive treatments.
-
White blood cell counts. Children with very high white blood cell counts need more intensive treatments. Commonly, white blood cell counts are labeled as very high if they are more than 50,000 per microliter (ml).
-
Immunophenotyping. This test shows the types and amounts of proteins made or expressed by the leukemia cells. Knowing if the cancer cells express the proteins more like those of normal white blood cells called B-cells or T-cells will help doctors plan appropriate treatment. It is also useful to help predict how well treatment will work.
-
Genetic abnormalities in the leukemia cells. Abnormal numbers of chromosomes, abnormal structural changes in a chromosome, or certain molecular genetic changes in the chromosomes of leukemia cells may affect outcome and treatment. Note that the genetic changes referred to here are changes in the genes of the leukemia cells, not the child’s cells – most children with leukemia have completely normal genes.
-
Response to early treatment. How well treatment works in the first 1 to 4 weeks of treatment may predict the leukemia’s overall response to treatment. This will be determined by examining the child’s blood or bone marrow regularly. Recent studies have shown that some children may need more intense treatment to improve the chance of a cure. This includes children whose cancer is not responding well to early treatment or those who have high levels of residual leukemia cells (cells remaining after treatment) at the end of remission induction (see Types of Treatment ).
Doctors also use the following terms to describe the state of ALL for each child:
Untreated ALL. The child has not yet received any treatment.
ALL in remission. There are normal levels of white cells and other blood cells after treatment. Physical examinations, blood counts, and bone marrow aspirations show no detectable leukemia. Remission is the absence of signs or symptoms of leukemia. However, it is very important to continue treatment, even when a child is in remission, to keep the leukemia from coming back.
Recurrent ALL. Recurrent ALL is leukemia that comes back after the child has had some period of remission. The leukemia may recur in the bone marrow, spinal fluid, testicles, or less commonly, in other areas of the body.
Refractory ALL. The leukemia did not go into remission, despite remission induction treatment (see more details in the next section on Types of Treatment .)
Information about the cancer’s classification will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment. You may use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Types of Treatment
ON THIS PAGE : You will learn about the different types of treatments doctors use for children with acute lymphoblastic leukemia (ALL). Use the menu to see other pages.
In general, cancer in children is uncommon. This means it can be hard for doctors to plan treatments unless they know what has been most effective in other children. That is why more than 60% of children with cancer are treated as part of a clinical trial. A clinical trial is a research study that tests a new approach to treatment. The “standard of care” is the best treatments known based on previous clinical trials. Clinical trials may test such approaches as a new drug, a new combination of existing treatments, or new doses of current therapies. The health and safety of all children participating in clinical trials are closely monitored.
To take advantage of these newer treatments, children with cancer should be treated at a pediatric cancer center or a cancer center with access to specialists in pediatric cancer. Doctors at these centers have extensive experience in treating children with cancer and have access to the latest research. A doctor who specializes in treating children with cancer is called a pediatric oncologist.
How childhood ALL is treated
In many cases, a team of doctors works with a child and the family to provide care. This is called a multidisciplinary team . Pediatric cancer centers often have extra support services for children and their families, such as child life specialists, nutritionists, physical and occupational therapists, social workers, and counselors. Special activities and programs to help your child and family cope may also be available.
Treatment options and recommendations depend on several factors, including the classification of ALL, possible side effects, and the patient’s preferences and overall health. Take time to learn about all of your child’s treatment options and be sure to ask questions about things that are unclear. Talk with your child’s doctor about the goals of each treatment and what your child can expect while receiving the treatment. These types of talks are called “shared decision-making.” Shared decision-making is when you and the doctors work together to choose treatments that fit the goals of your child’s care. Shared decision-making is particularly important for childhood ALL because there are different treatment options. Learn more about making treatment decisions .
Descriptions of common types of treatments used for childhood ALL are listed below. Your child's care plan also includes treatment for symptoms and side effects, an important part of cancer care.
The 3 types of treatments used to treat childhood ALL are chemotherapy, radiation therapy, and stem cell transplantation/bone marrow transplantation. All children with ALL receive chemotherapy. Some children will also need radiation therapy or stem cell transplantation/bone marrow transplantation.
-
Chemotherapy
-
Radiation therapy
-
Stem cell transplantation/bone marrow transplantation
-
Physical, emotional, and social effects of cancer
-
Remission and the chance of recurrence
-
If treatment does not work
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells.
A chemotherapy regimen, or schedule, usually consists of a specific number of cycles of drugs given over a set period of time. A patient may receive 1 drug at a time or combinations of different drugs given at the same time.
Chemotherapy is the primary treatment for ALL. It may be given by mouth (orally), injected into a vein or muscle, or injected into the cerebral spinal fluid (CSF). It is generally done in four phases:
-
Remission induction therapy uses chemotherapy to destroy as many of the leukemia cells as possible to cause the cancer to go into remission.
-
Central nervous system directed therapy destroys any leukemia cells in the central nervous system and prevents the spread of the disease to the spinal fluid.
-
Consolidation therapy begins when the child’s leukemia has gone into remission. Higher doses of chemotherapy, or drugs not used during previous treatment, are used to destroy most of the remaining leukemia cells.
-
Continuation or maintenance therapy lasts for two to three years to destroy any remaining (residual) leukemia cells.
The side effects of chemotherapy depend on the individual and the dose used, but they can include short-term side effects like hair loss, fatigue, loss of appetite, nausea and vomiting, diarrhea, and kidney and liver problems. If a drug called vincristine (Oncovin, Vincasar) is part of your child’s chemotherapy, there may be muscle weakness and nerve pain. These side effects usually go away after treatment is finished. Other side effects related to chemotherapy that may last longer or develop after treatment is finished include bone and joint problems and learning problems.
The severity of the side effects depends on the type and amount of the drug being given and the length of time the child receives the drug. The side effects each child experiences may also be affected by other factors, including biological differences in the way the medications are processed by the body, the child or teen’s age when diagnosed, and their overall health. That's why it is important to let your child's cancer care team know if your child is experiencing any changes in how they are feeling. Talk with your child's doctor regularly about what side effects are likely and how they can be managed.
Learn more about the basics of chemotherapy .
Return to top
Radiation therapy
Radiation therapy is the use of high-energy x-rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. The most common type of radiation treatment is called external-beam radiation therapy, which is radiation given from a machine outside the body. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
Radiation therapy for ALL is has recently been used when the leukemia has spread to the brain, spinal fluid, or the testicles, or in high-risk disease to help prevent the spread of leukemia to the spinal fluid. However, with current treatment regimens, radiation therapy is typically reserved for recurrent or refractory disease, and in some centers, patients with T-cell leukemia.
Side effects from radiation therapy may include hair loss, fatigue, mild skin reactions, upset stomach, and loose bowel movements. Talk with your child's doctor about what side effects may happen and how they can be managed. Most side effects go away soon after treatment is finished. However, long-term side effects of radiation treatment to the brain and body can occur and may possibly include hormone problems affecting growth and metabolism, learning problems, and an increased risk of developing a second cancer including a
brain tumor
,
skin
cancer,
salivary gland
cancer, and
thyroid
cancer can also occur after radiation treatment for ALL (see
Follow-up Care
).
Learn more about the basics of
radiation therapy
.
Return to top
Bone marrow transplantation/stem cell transplantation
Bone marrow/stem cell transplantation is most often used as a treatment for recurrent or refractory ALL. Rarely, transplantation may be recommended as part of the initial therapy when leukemia is associated with very high-risk features.
A bone marrow transplant is a medical procedure in which bone marrow that contains cancer is replaced by highly specialized cells. These cells, called hematopoietic stem cells, develop into healthy bone marrow. Hematopoietic stem cells are blood-forming cells found both in the bloodstream and in the bone marrow. This procedure is also called a stem cell transplant or hematopoietic stem cell transplant.
Before recommending transplantation, doctors will talk with the patient about the risks of this treatment. They will also consider several other factors, such as the type of cancer, results of any previous treatment, and the patient’s age and general health.
There are 2 types of hematopoietic stem cell transplantation depending on the source of the replacement blood stem cells: allogeneic (ALLO) and autologous (AUTO). ALLO uses donated stem cells, while AUTO uses the patient’s own stem cells. In both types, the goal is to destroy all of the cancer cells in the marrow, blood, and other parts of the body using high doses of chemotherapy and/or radiation therapy and then allow replacement blood stem cells to create healthy bone marrow.
Side effects depend on the type of transplant, your child’s general health, and other factors. Learn more about the basics of stem cell and bone marrow transplantation .
Return to top
Physical, emotional, and social effects of cancer
Leukemia and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your child’s care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Palliative care focuses on improving how your child feels during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after a cancer diagnosis. People who receive palliative care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. Your child may also receive palliative treatments similar to those meant to get rid of the cancer, such as chemotherapy or radiation therapy.
Before treatment begins, talk with your child’s doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative care options. Many patients also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
During treatment, your child’s health care team may ask you to answer questions about your child’s symptoms and side effects and to describe each problem. Be sure to tell the health care team if your child are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative care in a separate section of this website.
Return to top
Remission and the chance of recurrence
A remission is when leukemia cannot be detected in the body and there are no symptoms. This may also be called having “no evidence of disease” or NED.
A remission may be temporary or permanent. This uncertainty causes many people to worry that the leukemia will come back. While many remissions are permanent, it is important to talk with your child’s doctor about the possibility of the disease returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the leukemia does return. Learn more about coping with the fear of recurrence .
If the cancer returns after the original treatment, it is called recurrent ALL. If a recurrence happens, a new cycle of testing will begin again to learn as much as possible about it. After this testing is done, you and your child’s doctor will talk about treatment options. Often the treatment plan will include the treatments described above such as chemotherapy, radiation therapy, and/or stem cell transplantation but they may be used in a different combination or given at a different pace. Treatment of recurrent ALL depends on many factors, including the type of treatment the child received originally, the length of time between the initial diagnosis and the recurrence, and whether leukemia cells are found in the bone marrow, CSF, testicles, or in more than 1 of these sites when it recurs. Your child’s doctor may suggest clinical trials that are studying new ways to treat recurrent ALL. Just as for newly diagnosed patients, clinical trials typically offer the best chance of cure. Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects.
When ALL recurs, patients and their families often experience emotions such as disbelief or fear. Families are encouraged to talk with their health care team about these feelings and ask about support services to help them cope. Learn more about dealing with cancer recurrence .
Return to top
If treatment does not work
Although treatment is successful for many children with ALL, sometimes it is not. If a child’s leukemia cannot be cured or controlled, this is called advanced or terminal leukemia. This diagnosis is stressful, and advanced cancer may be difficult to discuss. However, it is important to have open and honest conversations with your child’s doctor and health care team to express your family’s feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families, and is there to help.
Hospice care is designed to provide the best possible quality of life for people who are expected to live less than 6 months. Parents and guardians are encouraged to talk with the health care team about hospice options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment can make staying at home a workable option for many families. Some children may be happier if they can attend school part-time or keep up other activities and social connections. The child’s health care team can help parents or guardians decide on an appropriate level of activity. Making sure a child is physically comfortable and free from pain is extremely important as part of end-of-life care. Learn more about caring for a terminally ill child and advanced cancer care planning .
The death of a child is an enormous tragedy, and families may need support to help them cope with the loss. Pediatric cancer centers often have professional staff and support groups to help with the process of grieving. Learn more on grieving the loss of a child.
Return to top
The next section in this guide is About Clinical Trials. It offers more information about research studies that are focused on finding better ways to care for children with cancer. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - About Clinical Trials
ON THIS PAGE : You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for children with acute lymphoblastic leukemia (ALL). To make scientific advances, doctors create research studies involving volunteers, called clinical trials. In fact, every drug that is now approved by the U.S. Food and Drug Administration (FDA) was previously tested in clinical trials.
Clinical trials are used for all types and stages of childhood ALL. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment.
Children who participate in clinical trials are often among the first to get a treatment before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. Parents are encouraged to talk with their child’s health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a long time after treatment. Talk with your child’s doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients and their families are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating children with ALL. Even if they do not benefit directly from the clinical trial, their participation may benefit future children with ALL.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about health insurance coverage of clinical trials
Sometimes people have concerns that, in a clinical trial, their child may receive no treatment by being given a placebo or a “sugar pill.” You and your child will always be told when a placebo is used in a study. Find out more about placebos in cancer clinical trials.
Patient safety and informed consent
To join a clinical trial, parents and children must participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options so that the person understands how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different from the risks of standard treatment.
-
Explain what will be required of each person in order to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.
-
Describe the purposes of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. Your child will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time for personal or medical reasons. This may include that the new treatment is not working or there are serious side effects. Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if they choose to leave the clinical trial before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all types of cancer. For specific topics being studied for leukemia, learn more in the Latest Research section.
Cancer.Net offers more information about cancer clinical trials in other areas of the website, including a complete section on clinical trials and places to search for clinical trials for a specific type of cancer .
In addition, you can find a free video-based educational program about cancer clinical trials, in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for childhood ALL. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about this type of cancer and how to treat it. Use the menu to see other pages.
Doctors are working to learn more about acute lymphoblastic leukemia (ALL), ways to treat it, how to best treat it, and how to provide the best care to children diagnosed with this disease. The following areas of research may include new options for patients through clinical trials. Always talk with your child’s doctor about the best diagnostic and treatment options for your child.
-
Monitoring leukemia recurrence. New methods for detecting small numbers of leukemia cells that can’t be seen under a microscope were introduced in the 1990s. These techniques are now being used to detect minimal residual disease (MRD) after remission. There are times when measurements of MRD, in blood or bone marrow samples, will be used to determine your child’s risk level and treatment. Research is ongoing to determine the level of MRD, measured at specific time point, that affects the rate of recurrence. Currently, researchers are studying the relationship between the biology of the leukemia cells and these measurements.
-
New treatments. Finding new ways to treat leukemia are important areas of research. New drugs to kill leukemia cells, such as the T-cell-specific drug nelarabine (Arranon), the antibody blinatumomab (Blincyto), and chimeric antigen receptor T-cells (CAR T-cells) are being studied and may improve the cure rate for children with ALL in the future. Other new treatments—antibodies, chemotherapy, and other biologically active treatments—are being studied with the hope that they will increase the cure rate and/or decrease the likelihood of side effects.
-
Palliative care/supportive care . Clinical trials are underway to find better ways of reducing symptoms and side effects of current childhood ALL treatments in order to improve comfort and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in childhood ALL, explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your child’s doctor or search online clinical trial databases .
-
Visit the Cancer.Net Blog to review research announced at recent scientific meetings about childhood cancer treatment and survivorship.
-
Visit the website of Conquer Cancer Foundation to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance in how to cope with the physical, emotional, social, and financial changes that cancer and its treatment can bring. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Coping with Treatment
ON THIS PAGE : You will learn more about coping with the physical, emotional, social, and financial side effects of childhood leukemia and its treatment. This page includes several links outside of this guide to other sections of this website. Use the menu to see other pages.
Every cancer treatment can cause side effects or changes to your child’s body and how they feel. For many reasons, people do not experience the same side effects even when given the same treatment for the same type of cancer. This can make it hard to predict how your child will feel during treatment.
As your family prepares to start cancer treatment, it is normal to fear treatment-related side effects after a diagnosis of leukemia. It may help to know that your child’s health care team will work to prevent and relieve side effects. Doctors call this part of cancer treatment palliative care or supportive care. It is an important part of your child’s plan, regardless of their age or the classification of the disease.
Coping with physical side effects
Common physical side effects from each treatment option for childhood acute lymphoblastic leukemia (ALL) are described within the Types of Treatment section. Learn more about side effects of cancer and its treatment, along with ways to prevent or control them . Changes to your child’s physical health depend on several factors, including the cancer’s stage, the length and dose of treatment, and your child’s general health.
It is important to discuss any new side effects or changes in existing side effects with your child’s health care team. Providing this information helps them find ways to treat or manage the side effects so your child feels more comfortable and can potentially keep any side effects from worsening.
You may find it helpful to keep track of your child’s side effects so you are prepared to talk about any changes with the health care team. Learn more about why tracking side effects is helpful .
Sometimes, physical side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment late effects . Treating long-term side effects and late effects is an important part of care for childhood cancer survivors. Learn more by reading the Follow-up Care section of this guide or talking with your child’s doctor.
Coping with emotional and social effects
Your family can have emotional and social effects after a cancer diagnosis. This may include dealing with a variety of emotions, such as anxiety, sadness, or anger, or managing stress. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about cancer.
You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your family’s needs.
Coping with the costs of cancer care
Cancer treatment can be expensive. It may be a source of stress and anxiety for people with cancer and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their cancer treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Coping with barriers to care
Some groups of people experience different rates of new cancer cases and experience different outcomes from their cancer diagnosis. These differences are called “cancer disparities.” Disparities are caused in part by real-world barriers to quality medical care and social determinants of health , such as where a person lives and whether they have access to food and health care. Cancer disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , older adults , and people who live in rural areas or other underserved communities .
If your child is having difficulty getting the care they need, talk with a member of the health care team or explore other resources that help support medically underserved people .
Talking with your child's health care team about side effects
Before starting treatment, talk with your child’s doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should we call about side effects?
Be sure to tell your child’s health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are not serious. This discussion should include physical, emotional, and social effects of cancer.
Caring for a child with cancer
Family members and friends play an important role in taking care of a child with ALL. This is called being a caregiver. As a parent or guardian, you are the primary caregiver for your child. However, friends and family members can give your family valuable support, even if they live far away.
When your child has ALL, you may have an additional range of responsibilities. These may include giving medications or managing symptoms and side effects. However, it is important to seek help from others. Below are some of the responsibilities your family or friends could help with:
-
Providing short-term care for your child
-
Giving support and encouragement
-
Assisting with meals or household chores
-
Helping with insurance and billing issues
A caregiving plan can help caregivers stay organized and help identify opportunities to delegate tasks to others. Ask how much care your child may need at home and with daily tasks during and after treatment. Use this 1-page fact sheet that includes an action plan to help make caregiving a team effort. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Managing Pain: Get this 36-page booklet about the importance of pain relief that includes a pain tracking sheet to record how pain affects your child. The free booklet is available as a PDF, so it is easy to print out.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on diarrhea and rash that provide a tracking sheet to record the timing and severity of the side effect. These free fact sheets are available as a PDF, so it is easy to print out.
The next section in this guide is Follow-up Care . It explains the importance of checkups after your child finishes cancer treatment. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Follow-Up Care
ON THIS PAGE: You will read about your child’s medical care after cancer treatment is finished and why this follow-up care is important. To see other pages, use the menu.
Care for children diagnosed with cancer does not end when active treatment has finished. Your child’s health care team will continue to check that the cancer has not come back, manage any side effects, and monitor your child’s overall health. This is called follow-up care. All children treated for cancer, including acute lymphoblastic leukemia (ALL), should have life-long, follow-up care.
Your child’s follow-up care may include regular physical examinations, medical test, or both. Doctors want to keep track of your child’s recovery in the months and years ahead. Patients should receive follow-up care regularly to monitor for the possible side effects listed in the Types of Treatment section of this guide for each treatment option, as well as for the risk of liver disease from chemotherapy or transfusion-related infection (both very rare) and the child's bone health. Talk with your child's doctor about possible side effects based on your child's specific treatment plan.
At first, check-ups will occur often. Then over time, these appointments will become more spread apart. Your child’s doctor can recommend the necessary screening tests to monitor their health. Follow-up care should address your child’s quality of life, including any developmental or emotional concerns.
Learn more about the importance of follow-up care .
Watching for recurrence
One goal of follow-up care is to check for a recurrence, which means that the cancer has come back. Cancer recurs because small areas of cancer cells may remain undetected in the body. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms.
During follow-up care, a doctor familiar with your child’s medical history can give you personalized information about the risk of recurrence. Your child's doctor will ask specific questions about your child’s health. Some children may have blood tests or imaging tests as part of regular follow-up care, but testing recommendations depend on several factors, including the type and classification of cancer originally diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results can add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects of childhood cancer
Sometimes, side effects may linger beyond the active treatment period. These are called long-term side effects. In addition, other side effects called late effects may develop months or even years after treatment has ended. Late effects can occur almost anywhere in the body. They include physical problems, such as heart problems , lung problems, and second cancers , which is a new type of cancer that happens in someone who has had cancer before. They can include problems with the patient's physical ability to have a child in the future, called infertility . They also include emotional problems, such as anxiety and depression , and problems with memory, thinking, and attention .
Based on the type of treatment your child received, the doctor will recommend what examinations and tests are needed to check for late effects. The possible long-term side effects associated with specific treatments are listed in the table below:
|
Type of Treatment |
Possible Late Effects |
|---|---|
|
Chemotherapy with cyclophosphamide (Cytoxan, Neosar) |
Secondary cancers Infertility (the physical inability to have children) |
|
Chemotherapy with types of drugs called anthracyclines, such as doxorubicin (Adriamycin) or daunorubicin (Cerubidine) |
Heart problems |
|
Radiation therapy |
Hormone problems affecting growth and metabolism Secondary cancers Infertility Learning problems |
|
High-dose chemotherapy or spinal fluid injections of chemotherapy like methotrexate (multiple brand names) and cytarabine (Cytosar-U) |
Learning problems |
|
Organ/Tissue Affected |
Type of Treatment |
Possible Late Effects |
|---|---|---|
|
Any tissue |
Radiation |
Benign and malignant (cancerous) tumors |
|
Bone marrow |
Chemotherapy with cyclophosphamide (Cytoxan, Neosar) and/or etoposide (VePesid, Toposar) |
Abnormal development of blood cells in the bone marrow (myelodysplasia); acute myeloid leukemia |
|
Bones |
Corticosteroids (prednisone, dexamethasone); methotrexate |
Weak bones (osteopenia, osteoporosis); Damage to bone joints (avascular necrosis) |
|
Brain |
Brain radiation High-dose chemotherapy or spinal fluid injections of chemotherapy like methotrexate (multiple brand names) and cytarabine (Cytosar-U) |
Problems with thinking skills affecting learning, attention |
|
Heart |
Chemotherapy with types of drugs called anthracyclines, such as doxorubicin (Adriamycin) or daunorubicin (Cerubidine) |
Weakening of heart muscle (cardiomyopathy) |
|
Kidney |
Methotrexate |
Reduced kidney function (usually short term effect seen during therapy) |
|
Liver |
Methotrexate |
Liver inflammation (usually short term effect during therapy) |
|
Nerves (peripheral) |
Vincristine |
Motor nerve weakness, sensory nerve injury causing tingling and numbness |
|
Pituitary gland |
Brain radiation |
Low levels of hormones important in growth, puberty and weight control |
|
Ovaries |
Cyclophosphamide |
Reduction of egg follicles; Infertility |
|
Testes |
Cyclophosphamide; testicular radiation |
Reduction of sperm count; Infertility |
Follow-up care should address your child’s quality of life, including any developmental or emotional concerns.
The Children's Oncology Group (COG) has studied the physical and psychological effects that childhood cancer survivors face. Based on these studies, COG has created recommendations for long-term follow-up care for childhood, adolescent, and young adult cancer survivors that can be found on a separate website: www.survivorshipguidelines.org .
Keeping a child’s personal health record
You are encouraged to organize and keep a personal record of the child’s medical information. The doctor will help you create this. That way, as the child enters adulthood, he or she has a clear, written history of the diagnosis, the treatments, and the doctor’s recommendations about the schedule for follow-up care. ASCO offers forms to help create a treatment summary to keep track of the cancer treatment your child received and develop a survivorship care plan when treatment is completed.
Some children continue to see their oncologist, while others transition back to the care of their pediatrician, primary care doctor, or another health care professional. This decision depends on several factors, including the type and classification of cancer, side effects, health insurance rules, and your family’s personal preferences. Talk with the health care team about your child’s ongoing medical care and any concerns you have about their future health.
If a doctor who was not directly involved in your child’s cancer care will lead the follow-up care, be sure to share the cancer treatment summary and survivorship care plan forms with him or her, and with all future health care providers. Details about the specific cancer treatment given are very valuable to the health care professionals who will care for your child throughout their lifetime.
The next section in this guide is Survivorship. It describes how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Survivorship
ON THIS PAGE : You will read about how to cope with challenges in everyday life after your child’s cancer diagnosis. Use the menu to see other pages.
What is survivorship?
The word “survivorship” means different things to different people, but it often describes living with, through, and beyond cancer. In some ways, survivorship is one of the most complicated parts of the cancer experience because it is different for every child and their family.
After active cancer treatment ends, children and their families may experience a mixture of strong feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after a cancer diagnosis. Other families stay very anxious about their child’s health and become uncertain about coping with everyday life.
One source of stress may occur when frequent visits to the health care team end after completing treatment. Often, relationships built with the cancer care team provide a sense of security during treatment, and children and their families miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, educational issues, emotional challenges, sexual development and fertility concerns, and/or financial issues.
Every family faces different concerns and challenges. With any challenge, a good first step is being able to recognize each fear and talk about it. Effective coping requires:
-
Understanding the challenge your family is facing,
-
Thinking through solutions,
-
Asking for and allowing the support of others, and
-
Feeling comfortable with the course of action your family chooses.
It may be helpful to join an in-person support group or online community of childhood cancer survivors. Support groups also exist for parents of children diagnosed with cancer. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of the health care team, individual counseling, or asking for assistance at the learning resource center of the place where your child received treatment.
Healthy living after cancer
Survivorship often serves as a strong motivator to make lifestyle changes, often for the family as a whole.
Children who have had cancer can enhance the quality of their future by following established guidelines for good health into and through adulthood, including not smoking, limiting alcohol, maintaining a healthy weight, eating well, managing stress, and participating in regular physical activity. Talk with the doctor about developing a plan that is best for your child’s needs. Learn more about making healthy lifestyle choices .
As they get older, survivors should carefully monitor their level of functioning and level of stress, and they may need counseling if they have any problems or challenges. It is important that children who have trouble with school have neuropsychological testing (testing of thinking skills by a psychologist) to find the cause. Based on the results, the psychologist can advise teachers about changes that can be made in the classroom or teaching plan to help the child learn. Survivors should also be evaluated for bone or joint pain that may result from bone cell death caused by cancer treatments that reduce blood flow in bone joints. The website of the Children’s Oncology Group provides recommendations for follow-up care (Please note this link takes you to a separate website.)
Childhood cancer survivors should also think about their needs for follow-up care when considering their available choices for health insurance. This Cancer.Net article outlines the basics of Cancer and Affordable Care Act .
It is important that your child has recommended medical checkups and tests (see Follow-up Care ) to take care of their health. Cancer rehabilitation may be recommended, and this could mean any of a wide range of services such as physical therapy, family or individual counseling, nutritional planning, and/or educational assistance. The goal of rehabilitation is to help survivors and their families regain control over many aspects of their lives and remain as independent and productive as possible.
Talk with the doctor to develop a survivorship care plan that is best for your child’s needs.
Changing role of caregivers
Parents, other family members, and friends may also go through periods of transition. A caregiver plays a very important role in supporting a child diagnosed with cancer, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to a child’s cancer diagnosis will become much less or come to an end as your child gets older. Family counselors at pediatric cancer centers can help with this transition. You can also learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about cancer survivorship, explore these related items. Please note these links will take you to other sections of Cancer.Net:
-
Survivorship Resources : Cancer.Net offers a lot of information and resources to help survivors cope, including specific sections for children , teens , and young adults . There is also a main section on survivorship for people of all ages.
-
ASCO Answers Guide to Cancer Survivorship : Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. The free booklet is available as a PDF so it is easy to print out.
The next section offers Questions to Ask the Health Care Team to help start conversations with your child’s cancer care team. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask the doctor or other members of the health care team, to help you better understand your child’s diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your child’s health care. These suggested questions are a starting point to help you learn more about your child’s cancer care and treatment. You are also encouraged to ask additional questions that are important to you and your family. You may want to print this list and bring it to your child’s next appointment, or download Cancer.Net’s free mobile app for a digital list and other interactive tools to manage your child’s care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask after getting a diagnosis
-
What type of leukemia does my child have?
-
Can you explain my child’s pathology report (laboratory test results) to me?
-
Will more tests be needed to confirm the diagnosis?
-
What are the results of the analysis of the spinal fluid? What does this mean?
-
What are the results of the bone marrow aspiration? What does this mean?
-
What are the results of the cytogenetic studies done? What does this mean?
Questions to ask about choosing a treatment and managing side effects
-
What are the treatment options?
-
What is the goal of each treatment? Is it to eliminate the cancer, help my child feel better, or both?
-
What clinical trials are open to my child? Where are they located, and how do I find out more about them?
-
What treatment plan do you recommend? Why?
-
Who will be part of my child’s health care team, and what does each member do?
-
Who will be coordinating my child’s overall treatment?
-
What are the possible side effects of this treatment, both in the short term and the long term?
-
Could this treatment affect my child’s ability to become pregnant or have children in the future? If so, should I talk with a fertility specialist before treatment begins?
-
What can I do to protect my child from infection during and after treatment?
-
When should I call the doctor or hospital if there is a problem while at home with my child?
-
How will this treatment affect my child’s daily life? Will he or she be able to attend school and perform their usual activities?
-
If I’m worried about managing the costs related to my child’s cancer care, who can help me with these concerns?
-
What support services are available to my child? To my family?
-
If I have questions or problems, who should I call?
Questions to ask about planning follow-up care
-
What follow-up tests will my child need, and how often will he or she need them?
-
Are there blood tests or check-ups that can be done closer to home?
-
What long-term side effects or late effects are possible based on the treatment my child received?
-
What can be done to prevent or relieve the side effects?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
What survivorship support services are available to my child? To my family?
-
Whom should I call for questions or problems?
The next section in this guide is Additional Resources . It offers some more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Leukemia - Acute Lymphoblastic - ALL - Childhood - Additional Resources
ON THIS PAGE : You will find some helpful links to other areas of Cancer.Net that provide information about cancer care and treatment. This is the final page of Cancer.Net’s Guide to Childhood Acute Lymphoblastic Leukemia (ALL). Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of cancer for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Search for a cancer specialist in your local area using this free database of doctors from the American Society of Clinical Oncology.
-
Learn what medical phrases and terms used in cancer care and treatment mean.
-
Read more about the first steps to take when your child is diagnosed with cancer .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of cancer care.
-
Learn more about coping with the emotions that cancer can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for children with this type of cancer.
-
Explore what to do when your child finishes active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
-
Watch Cancer.Net videos with ASCO experts explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
This is the end of Cancer.Net’s Guide to Childhood ALL. Use the menu to choose a different section to read in this guide.