













Breast Cancer - Introduction
ON THIS PAGE: You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Breast Cancer. Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
Anyone can develop breast cancer. In the United States, breast cancer is the most common cancer in women (excluding skin cancer). Male breast cancer is rare, accounting for less than 1% of all breast cancers. Learn more about male breast cancer in a separate guide on this website .
About the breast
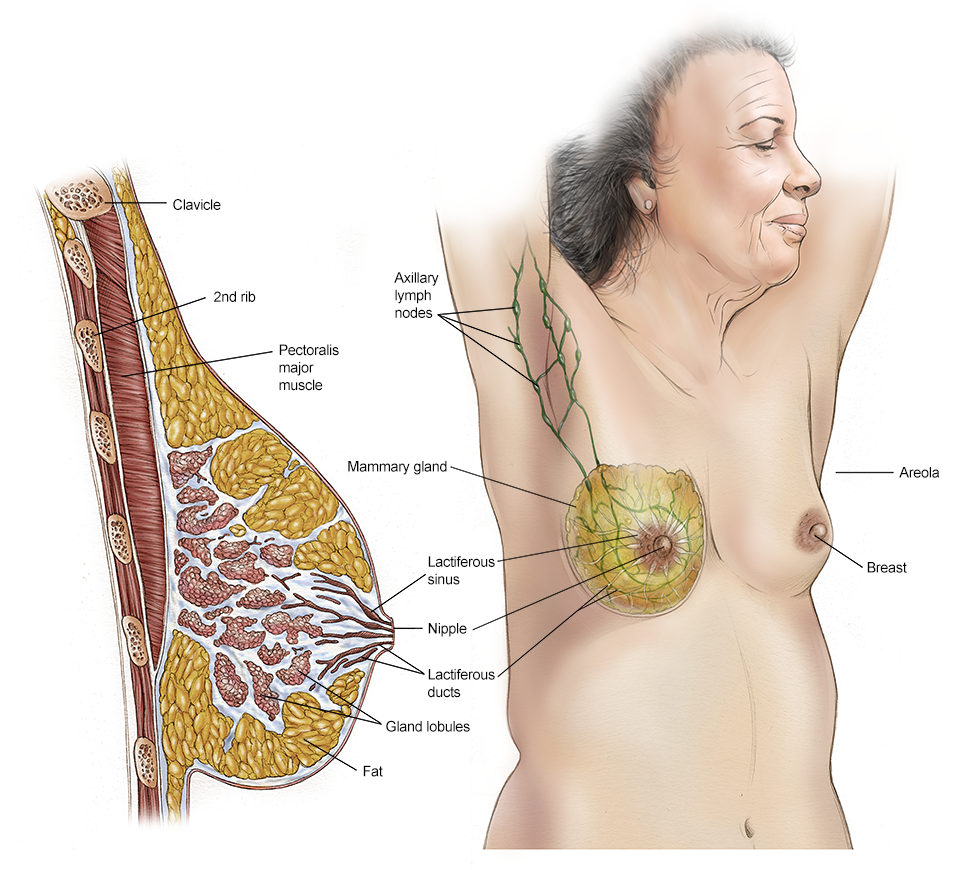
The breast is made up of different tissues, ranging from very fatty tissue to very dense tissue. Within this tissue is a network of lobes. Each lobe is made up of small, tube-like structures called lobules that contain milk glands. Small ducts connect the glands, lobules, and lobes, carrying milk from the lobes to the nipple. The nipple is located in the middle of the areola, which is the darker area that surrounds the nipple.
Blood and lymph vessels also run throughout the breast. Blood vessels nourish the cells by delivering oxygen and nutrients and also removing waste and carbon dioxide. Lymph vessels, unlike blood vessels, only carry fluid away from tissues. They connect to lymph nodes and the lymphatic system, which drains bodily waste products. Lymph nodes are the small, bean-shaped organs that are part of the body's immune system and help fight infection. Groups of lymph nodes are located in different areas throughout the body, such as in the neck, groin, and abdomen. Regional lymph nodes of the breast are those nearby the breast, such as the lymph nodes under the arm, which are called axillary lymph nodes.
About breast cancer
Cancer begins when healthy cells in the breast change and grow out of control, forming a mass or sheet of cells called a tumor. A tumor can be cancerous or noncancerous, also called benign. A cancerous tumor is malignant, meaning it can grow and spread to other parts of the body. A benign tumor means the tumor can grow but has not spread.
This guide covers both non-invasive (stage 0) as well as early-stage and locally advanced invasive breast cancer, which includes stages I, II, and III. The stage of breast cancer describes how much the cancer has grown, and if or where it has spread.
Although breast cancer most commonly spreads to nearby lymph nodes, in which case the breast cancer is still considered a local or regional disease, it can also spread further through the body through the blood vessels and/or lymph nodes to areas such as the bones, lungs, liver, and brain. This is called metastatic or stage IV breast cancer and is the most advanced stage of the disease. However, the involvement of nearby lymph nodes alone is generally not stage IV breast cancer. Learn more about metastatic breast cancer in a separate guide on this website.
If breast cancer comes back after initial treatment, it can recur locally, meaning in the same breast and/or regional lymph nodes. It can also recur elsewhere in the body, called a distant recurrence or metastatic recurrence .
Types of breast cancer
Breast cancer can be invasive or non-invasive. Invasive breast cancer is cancer that spreads into surrounding tissues and/or distant organs. Non-invasive breast cancer does not go beyond the milk ducts or lobules in the breast. About 80% of breast cancer is invasive cancer, and about 20% is non-invasive cancer. There are multiple types of breast cancers, which are classified based on how they look under a microscope.
-
Ductal carcinoma in situ (DCIS). This is a non-invasive cancer (stage 0) that is located only in the duct and has not spread outside the duct.
-
Invasive or infiltrating ductal carcinoma. This is cancer that has spread outside of the ducts. It is the most common type of invasive breast cancer.
-
Invasive lobular carcinoma. This is a type of breast cancer that has spread outside of the lobules.
Less common types of invasive breast cancer include:
-
Medullary
-
Mucinous
-
Tubular
-
Metaplastic
-
Papillary
-
Micropapillary
-
Apocrine
-
Inflammatory breast cancer , which is an aggressive type of cancer that accounts for about 1% to 5% of all invasive breast cancers.
Paget’s disease is a rare type of cancer in the skin of the nipple or in the skin closely surrounding the nipple. It begins in the ducts of the nipple, then spreads to the nipple surface and the areola (dark circle of skin around the nipple). The nipple and areola often become scaly, red, itchy, and irritated. Often, Paget's disease is mistaken for eczema or an infection before the correct diagnosis is made. Although it is usually non-invasive, it can also be an invasive cancer. It is usually found with an underlying breast cancer.
Breast cancer subtypes
There are 3 main subtypes of breast cancer that are determined by doing specific tests on a sample of the tumor to determine its characteristics. These tests will help your doctor learn more about your cancer and recommend the most effective treatment plan .
Testing the tumor sample can find out if the cancer is:
-
Hormone receptor positive. Breast cancers expressing estrogen receptors (ER) and/or progesterone receptors (PR) are called “hormone receptor positive.” These receptors are proteins found in cells. Tumors that have estrogen receptors are called “ER positive.” Tumors that have progesterone receptors are called “PR positive.” Only 1 of these receptors needs to be positive for a cancer to be called hormone receptor positive. This type of cancer may depend on the hormones estrogen and/or progesterone to grow. Hormone receptor-positive cancers can occur at any age, but they are more common after menopause. About two-thirds of breast cancers have estrogen and/or progesterone receptors. Cancers without these receptors are called “hormone receptor negative.” Hormone receptor-positive breast cancers are commonly treated using hormone therapy (see Types of Treatment ).
-
HER2 positive. About 15% to 20% of breast cancers depend on the gene called human epidermal growth factor receptor 2 ( HER2 ) to grow. These cancers are called “HER2 positive” and have many copies of the HER2 gene or high levels of the HER2 protein. These proteins are also called “receptors.” The HER2 gene makes the HER2 protein, which is found on the cancer cells and is important for tumor cell growth. HER2-positive breast cancers grow more quickly. They can also be either hormone receptor positive or hormone receptor negative. HER2-positive early stage breast cancers are commonly treated using HER2-targeted therapies (see Types of Treatment ). Cancers that have no HER2 protein are called “HER2 negative." Cancers that have low levels of the HER2 protein and/or few copies of the HER2 gene are sometimes now called “HER2 low."
-
Triple negative. If a tumor does not express ER, PR, and HER2, the tumor is called “triple negative.” Triple-negative breast cancer makes up about 10% to 20% of invasive breast cancers. Triple-negative breast cancer seems to be more common among younger women, particularly younger Black women and Hispanic women. Triple-negative breast cancer is also more common in women with a mutation in the BRCA1 gene. Experts often recommend that people with triple-negative breast cancer be tested for BRCA gene mutations. See the Risk Factors and Prevention section for more information on these genetic mutations.
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to other sections on Cancer.Net:
-
ASCO Answers Fact Sheet: Read a 1-page fact sheet that offers an introduction to breast cancer. This free fact sheet is available as a PDF, so it is easy to print.
-
ASCO Answers Guide : Get this 52-page booklet that helps you better understand breast cancer and its treatment options. This free booklet is available as a PDF, so it is easy to print.
-
Cancer.Net Blog: Read an ASCO expert’s opinion about what newly diagnosed patients should know about breast cancer.
-
Cancer.Net En Español: Read about breast cancer in Spanish . Infórmase sobre cáncer de mama en español .
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with breast cancer and general survival rates. Use the menu to choose a different section to read in this guide.
Breast Cancer - Statistics
ON THIS PAGE: You will find information about the estimated number of people who will be diagnosed with breast cancer each year. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with cancer are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this cancer and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for you individually. The original sources for these statistics are provided at the bottom of this page.
How many people are diagnosed with breast cancer?
Worldwide, female breast cancer has now surpassed lung cancer as the most commonly diagnosed cancer. An estimated 2,261,419 new cases of breast cancer were diagnosed in women across the world in 2020.
More women in the United States are diagnosed with breast cancer than any other type of cancer, besides skin cancer. The disease accounts for 1 in 3 of new female cancers annually.
In 2023, an estimated 297,790 women in the United States will be diagnosed with invasive breast cancer, and 55,720 women will be diagnosed with non-invasive (in situ) breast cancer. From the mid-2000s, invasive breast cancer in women has increased by approximately half a percent each year. This is likely caused by an increase in excess body weight in women overall, as well as a drop in fertility rates and rising age for first births. An estimated 2,800 men in the United States will be diagnosed with invasive breast cancer in 2023.
Currently, there are more than 3.8 million women who are living with or beyond breast cancer in the United States.
It is estimated that 43,700 deaths (43,170 women and 530 men) from breast cancer will occur in the United States in 2023. Worldwide, female breast cancer is the fifth leading cause of death. In 2020, an estimated 684,996 women across the world died from breast cancer.
Breast cancer is the second most common cause of death from cancer in women in the United States after lung cancer. However, the number of women who have died of breast cancer has decreased by 43% since 2020 following a peak in 1989. This is thanks to early detection, treatment improvements, and greater breast cancer awareness. As a result, more than 460,000 breast cancer deaths were prevented during that period. Although Black women are diagnosed less often with breast cancer than White women, they have a 40% higher death rate from the disease.
Breast cancer typically is diagnosed in middle-aged and older women. The median age of diagnosis is 63. Although it is not common, some women diagnosed with the disease are under age 45. Black women are more likely to develop breast cancer before the age of 40 compared to White women.
What is the survival rate for breast cancer?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from breast cancer. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having cancer may affect life expectancy. Relative survival rate looks at how likely people with breast cancer are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this cancer.
Example: Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for people with breast cancer are only an estimate. They cannot tell an individual person if cancer will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for women in the United States with non-metastatic invasive breast cancer is 91%. The 10-year relative survival rate for women with non-metastatic invasive breast cancer is 85%.
The survival rates for breast cancer vary based on several factors. These include the stage of cancer, a person’s age and general health, and how well the treatment plan works.
If the invasive breast cancer is located only in the breast, the 5-year relative survival rate of women with this disease is 99%. About 66% of women with breast cancer are diagnosed at this stage. Adolescent and young adult females ages 15 to 39 in the United States are less likely to be diagnosed at an early stage of breast cancer (47% of cases in this age group) compared to women older than 65 (68% of cases in this age group). Black women are also less likely to be diagnosed at an early stage (57% of cases in this group) compared to White women (68% of cases in this group).
If the cancer has spread to the regional lymph nodes, the 5-year relative survival rate is 86%. If the cancer has spread to a distant part of the body, the 5-year relative survival rate is 30%. The relative survival rate for breast cancer is 9% lower in Black women compared to White women.
Six percent (6%) of women have cancer that has spread outside of the breast and regional lymph nodes at the time they are first diagnosed with breast cancer. This is called "de novo" metastatic breast cancer. Even if the cancer is found at a more advanced stage, new treatments help many people with breast cancer maintain a good quality of life for some time. Learn more about metastatic breast cancer in a separate guide on this website .
Experts measure relative survival rate statistics for breast cancer every 5 years. This means the estimate may not reflect the results of advancements in how breast cancer is diagnosed or treated from the last 5 years. Talk with your doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's publications, Cancer Facts & Figures 2023 and Cancer Facts & Figures 2020; the ACS website ; the International Agency for Research on Cancer website; and the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) Program. (All sources accessed February 2023.)
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by breast cancer. Use the menu to choose a different section to read in this guide.
Breast Cancer - Medical Illustrations
ON THIS PAGE: You will find a drawing of the main body parts affected by breast cancer. Use the menu to see other pages.
The next section in this guide is Risk Factors and Prevention . It describes the factors that may increase the chance of developing breast cancer. Use the menu to choose a different section to read in this guide.
Breast Cancer - Risk Factors and Prevention
ON THIS PAGE: You will find out more about the factors that increase the chance of developing breast cancer. Use the menu to see other pages.
A risk factor is anything that increases a person’s chance of developing cancer. Although risk factors often influence the development of cancer, most do not directly cause cancer. Some people with several risk factors never develop cancer, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed lifestyle and health care choices.
Most breast cancers are sporadic, meaning they develop from damage to a person’s genes that occurs by chance after they are born. Sporadic breast cancer means there is no risk of the person passing the gene on to their children. The underlying cause of sporadic breast cancer is a combination of internal, or hormonal, exposures; lifestyle factors; environmental factors; and normal physiology, such as DNA replication.
Inherited breast cancers are less common, making up about 10% of cancers. Inherited breast cancer occurs when gene changes, called mutations or alterations, are passed down within a family from parent to child. Many of those mutations are in tumor suppressor genes, such as BRCA1, BRCA2, and PALB2 . These genes normally keep cells from growing out of control and turning into cancer. But when these cells have a mutation, it can cause them to grow out of control.
When considering your breast cancer risk, it is important to remember that a high majority of people who develop breast cancer have no obvious risk factors and no strong family history of breast cancer. Multiple risk factors influence the development of breast cancer. This means that all people need to be aware of changes in their breasts. They also need to talk with their doctor about recommendations for receiving regular breast examinations by a doctor as well as mammograms . A mammogram is an x-ray of the breast that can often find a tumor that is too small to be felt.
The following factors may raise a person’s risk of developing breast cancer:
Age. The risk of developing breast cancer increases with age, with most cancers developing after age 50. The median age for developing breast cancer is 63.
Personal history of breast cancer. A woman who has had breast cancer in 1 breast has a higher risk of developing a new cancer in the other breast.
Family history of breast cancer. Breast cancer may run in the family in any of these situations:
-
1 or more women are diagnosed with breast cancer at age 45 or younger
-
1 or more women are diagnosed with breast cancer before age 50 with an additional family history of cancer, such as ovarian cancer , metastatic prostate cancer , and pancreatic cancer
-
There are breast and/or ovarian cancers in multiple generations on 1 side of the family, such as having both a grandmother and an aunt on the father’s side of the family who were both diagnosed with 1 of these cancers
-
A woman in the family is diagnosed with a second breast cancer in the same or the other breast or has both breast and ovarian cancer
-
A relative is diagnosed with male breast cancer
-
Having Ashkenazi Jewish ancestry
It is important to talk with your doctor if your family has experienced any of the above situations. It could be a sign that your family carries an inherited breast cancer genetic mutation, such as
BRCA1,
BRCA2,
or
PALB2
(see "Inherited risk/genetic disposition," below).
When looking at family history, it’s also important to consider your father’s side of the family. Your father’s side is equally important as your mother’s side in determining your personal risk for developing breast cancer.
Inherited risk/genetic predisposition.
There are several inherited genetic mutations linked with an increased risk of breast cancer, as well as other types of cancer.
BRCA1
or
BRCA2
are the most common known genes linked to breast cancer. Mutations in these genes are linked to an increased risk of breast and ovarian cancers, as well as other types of cancer.
Male breast cancer
, as well as the risk for prostate cancer and other cancers, is also increased if there is a mutation in 1 of these genes. Learn more about hereditary breast and ovarian cancer in a
more detailed guide
on this website.
Other gene mutations or hereditary conditions can increase a person’s risk of breast cancer. They are far less common than
BRCA1
or
BRCA2
, and they do not increase the risk of breast cancer as much. Some of these genes and syndromes are:
-
Lynch syndrome , linked with the MLH1 , MSH2, MSH6, and PMS2 genes
-
Cowden syndrome (CS) , linked with the PTEN gene
-
Li-Fraumeni syndrome (LFS) , linked with the TP53 gene
-
Peutz-Jeghers syndrome (PJS) , linked with the STK11 gene
-
Ataxia telangiectasia (A-T) , linked with the ATM gene
-
Hereditary diffuse gastric cancer , linked with the CDH1 gene
-
PALB2 gene
-
CHEK2 gene
There are also other genes that may cause an increased risk of breast cancer. More research is needed to understand how they increase a person’s risk. For example, a person can inherit a gene mutation but not develop breast cancer. Research is also ongoing to find other genes that may affect breast cancer risk.
Genetic testing
through blood or saliva tests is available to test for known mutations in
BRCA1
and
BRCA2
genes and other genes linked with hereditary syndromes. Ask your doctor if genetic testing is recommended for you. Your doctor may recommend a test called a “panel test.” A panel test looks for mutations in several different genes at the same time. There are different panel tests your doctor can recommend. However, these tests are not recommended for everyone, and it is recommended that people receive appropriate
genetic counseling
before
undergoing testing to make sure they have the right test performed, and so they understand the results of the tests.
There are tests that a person can request directly from a testing company that do not require a doctor's order. These are generally done by using a kit sent through the mail. If you choose to have one of these tests performed, you should discuss it with your doctor first, as some tests only evaluate a limited number of genes. This means they may provide incomplete information, and you may need may need a different test performed to check all the genes that may be important for you based on your family history. In addition, you may need repeat testing to confirm that the results are correct. Learn more about the basics of
genetic testing for cancer risk
.
If a person learns they have a genetic mutation, there may be steps they can take to lower their risk of breast and ovarian cancers (see "Prevention," below). They may need a different breast cancer screening schedule than the general population, such as having additional types of tests or starting screening at a younger age. In addition, they may need different types of screening tests for other cancers, such as having a colonoscopy at a younger age to detect colorectal cancer.
Personal history of ovarian cancer. BRCA1 and BRCA2 gene mutations greatly increase the risk of both ovarian cancer and breast cancer . Therefore, a person diagnosed with hereditary ovarian cancer caused by a BRCA gene mutation have an increased risk of breast cancer as well. Mutations in other genes, such as PALB2, RAD51C, and RAD51D, are also associated with increased risk of ovarian cancer and breast cancer. Women with breast cancer who did not inherit a mutation in one of these genes generally do not have a higher risk of ovarian cancer.
Early menstruation and late menopause. If menstruation began before ages 11 or 12 or menopause began after age 55, there is a somewhat higher risk of breast cancer. This is because the breast cells have been exposed to estrogen and progesterone for a longer time. Estrogen and progesterone are hormones that control the development of secondary sex characteristics, such as breast development, and pregnancy. The production of estrogen and progesterone decreases with age, with a steep decrease around menopause. Longer exposure to these hormones increases breast cancer risk.
Timing of pregnancy. Having a first pregnancy after age 35 or if you've never had a full-term pregnancy brings a higher risk of breast cancer. Pregnancy may help protect against breast cancer because it pushes breast cells into their final phase of maturation.
Hormone replacement therapy after menopause. Using hormone therapy with both estrogen and progestin after menopause, often called hormone replacement therapy, within the past 5 years or for several years increases the risk of breast cancer. In fact, the number of new breast cancers diagnosed has dropped substantially as there is now less use of postmenopausal hormone therapy. However, women who have taken only estrogen, without previously receiving progestin, for up to 5 years (because they had their uterus removed for other reasons) appear to have a slightly lower risk of breast cancer.
Oral contraceptives or birth control pills. Some studies suggest that oral contraceptives to prevent pregnancy slightly increase the risk of breast cancer, while others have shown no link between the use of oral contraceptives and development of breast cancer. Research on this topic is ongoing.
Race and ethnicity.
Breast cancer is the most common cancer diagnosis in women, other than skin cancer, regardless of race. White women are more likely to develop breast cancer than Black women, but among women younger than 45, the disease is more common in Black women than in White women. Black women are also more likely to die from the disease. Reasons for survival differences may include differences in biology, other health conditions, and socioeconomic factors affecting access to medical care.
Women of Ashkenazi or Eastern European Jewish heritage also have an increased risk of breast cancer because they may be more likely to have inherited a
BRCA1
gene mutation. Breast cancer is least commonly diagnosed in Hispanic, Asian/Pacific Islander, and American Indian/Alaska Native women. Both Black women and Hispanic women are more likely to be diagnosed with larger tumors and later-stage cancer than White women. However, Hispanic women generally have better survival rates than White women. Breast cancer diagnoses have been increasing in second generation Asian/Pacific Islander and Hispanic women for unclear reasons. However, the increase is likely related to changes in diet and lifestyle associated with living in the United States.
Atypical hyperplasia of the breast. This diagnosis increases the risk of developing breast cancer in the future. It is characterized by abnormal, but not cancerous, cells found in a biopsy (see Diagnosis ) of the breast.
Lobular carcinoma in situ (LCIS). LCIS refers to abnormal cells found in the lobules or glands of the breast. It is not considered cancer. However, LCIS in 1 breast increases the risk of developing invasive breast cancer in either breast in the future. If LCIS is found during a biopsy (see Diagnosis ), it may be removed to check for other changes. Talk with your doctor about the best way to monitor and treat this condition.
Breast density. Having dense breast tissue generally means you have more milk glands, milk ducts, and supportive tissue in the breast than fatty tissue. Dense breast tissue is a measure used to describe mammogram images as opposed to how the breast feels. Breast density usually decreases with age. Having dense breast tissue increases the risk of developing breast cancer. In addition, dense breast tissue may make it more difficult to detect a tumor on standard imaging tests, such as mammography (see Diagnosis ). Some states require that mammogram results include information about breast density if the results show that a person has dense breast tissue. However, at this time, there are no special screening guidelines for people with dense breasts.
Lifestyle factors. As with other types of cancer, studies continue to show that various lifestyle factors may contribute to the development of breast cancer.
-
Weight. Recent studies have shown that being post-menopausal and being overweight or obese brings an increased risk of breast cancer. There is also a higher risk of the cancer coming back after treatment.
-
Physical activity. A lower amount of physical activity is associated with an increased risk of developing breast cancer and a higher risk of having the cancer come back after treatment.
-
Alcohol. Current research suggests that having more than 1 to 2 servings of alcohol , including beer, wine, and spirits, per day raises the risk of breast cancer. General recommendations are typically to limit your alcohol intake to 3 to 4 servings per week.
-
Food. There is no reliable research that confirms that eating or avoiding specific foods increases the risk of developing breast cancer or having the cancer come back after treatment. However, eating more fruits and vegetables and fewer animal fats is linked with many health benefits, including a slight decrease in the risk of breast cancer.
Socioeconomic factors. More affluent women in all racial and ethnic groups have a higher risk of developing breast cancer than less affluent women in the same groups. These differences may be due to variations in diet, pregnancy factors such as age at first pregnancy and number of pregnancies, and other risk factors. Women living in poverty are more likely to be diagnosed at an advanced stage and are less likely to survive the disease than more affluent women. This is likely due to multiple factors, including lifestyle factors and other health conditions such as obesity and tumor biology. Access to health care and the availability of treatment play additional roles.
Radiation exposure at a young age.
Exposure to ionizing radiation at a young age may increase a woman’s risk of breast cancer. For example, therapeutic radiation to the chest for
Hodgkin lymphoma
may increase breast cancer risk in both breasts.
The very small amount of radiation a person receives during a mammogram has not been linked to an increased risk of breast cancer.
Understanding your risk of breast cancer
Several breast cancer risk assessment tools have been developed to help people estimate their chance of developing breast cancer. The best studied is the Gail model, which is available on the National Cancer Institute’s website at www.cancer.gov/bcrisktool . After you enter some personal and family information, including your race/ethnicity, the tool provides you with a 5-year and lifetime estimate of the risk of developing invasive breast cancer. Because it only asks for information about breast cancer in first-degree family members and does not include their ages at diagnosis, the tool works best at estimating risk in people without a strong inherited breast cancer risk. In addition, it cannot be used by patients who have a personal history of breast cancer to determine their risk of developing a new breast cancer. For people with a personal history of breast cancer or a strong family history of breast cancer, other ways of determining their risk of breast cancer may work better. People with a strong family history of breast cancer risk should consider talking to a genetic counselor .
It is important to talk with your doctor about how to estimate your personal risk of breast cancer and to discuss risk-reducing or prevention options (see below).
Prevention
Different factors cause different types of cancer. Researchers continue to look into what factors cause breast cancer, and how to prevent it. Although there is no proven way to completely prevent breast cancer, you may be able to lower your risk.
For those at higher risk, the following options may help reduce your risk of breast cancer. Talk with your health care team for more information about your personal risk of breast cancer.
Lifestyle choices to lower cancer risk
One way to lower your risk of breast cancer is by getting regular physical activity. Studies suggest that 30 to 60 minutes per day of moderate- to high-intensity physical activity is associated with a lower breast cancer risk. Other ways to lower your risk include staying at a healthy weight and avoiding the use of hormone replacement therapy with both estrogen and progestin after menopause. Breastfeeding may also reduce breast cancer risk. Learn about more lifestyle choices that may help lower your risk of breast cancer .
Surgery to lower cancer risk
When there is a BRCA1 or BRCA2 genetic mutation present, which substantially increases the risk of breast cancer, preventive removal of the breasts may be considered. This procedure is called a prophylactic mastectomy. It appears to reduce the risk of developing breast cancer by at least 90% to 95%. People with these genetic mutations should also consider the preventive removal of the ovaries and fallopian tubes, called a prophylactic salpingo-oophorectomy. This procedure can reduce the risk of developing ovarian cancer, and possibly breast cancer, by stopping the ovaries from making estrogen. When considering having these procedures, it is important to talk with your doctor about possible physical and emotional side effects.
Drugs to lower cancer risk
If you have a higher than usual risk of developing breast cancer, consider talking with your doctor about drugs that may help prevent breast cancer. This approach is called "chemoprevention." For breast cancer, this is the use of hormone-blocking drugs to reduce cancer risk.
-
Tamoxifen (available as a generic drug). Tamoxifen is a type of drug called a selective estrogen receptor modulator (SERM). It is often used as a treatment for breast cancer for people who already have the disease. Tamoxifen blocks the effects of estrogen on tumor growth.
Tamoxifen may be an option to help lower the risk of breast cancer, specifically ER-positive breast cancer, for women who are age 35 or older. Research has shown that it may also be effective to reduce the risk of breast cancer and cause minimal side effects for women with non-invasive breast cancer (also called ductal carcinoma in situ, or DCIS) or precancerous breast conditions called LCIS or atypical hyperplasia of the breast. It is not recommended for those with a history of blood clots, stroke, or who are immobilized (unable to move around) for a long time. It is also not recommended during pregnancy or if you are trying to become pregnant, or during breastfeeding. The side effects of tamoxifen may include hot flashes, vaginal discharge, sexual side effects, mood changes, and a higher risk of developing uterine cancer, blood clots, and stroke.
-
Raloxifene (available as a generic drug). Raloxifene is also a SERM. It is often used to prevent osteoporosis (thinning of the bones) after menopause.
Raloxifene may be an option after the age of 35 when there is a higher risk of breast cancer and after menopause. Raloxifene can be used for longer than 5 years and may reduce the risk of bone loss in addition to lowering breast cancer risk. It is not recommended for women who have not been through menopause or who have a history of blood clots, stroke, or are immobilized for a long time.
The side effects of raloxifene may include hot flashes, leg cramps, swelling of the legs and arms, weight gain, stroke, blood clots, vaginal dryness, and pain during sexual intercourse. Women taking raloxifene are less likely to develop blood clots, uterine problems, and cataracts than people taking tamoxifen.
-
Aromatase inhibitors (AIs). AIs reduce the amount of estrogen in the body by blocking estrogen production. There are 3 AIs that may be options for lowering breast cancer risk after menopause when there is a higher risk of developing breast cancer: exemestane (Aromasin), anastrozole (Arimidex), and letrozole (Femara). While they are only approved by the U.S. Food and Drug Administration (FDA) for use in breast cancer treatment and not in the risk-reduction setting, large, randomized clinical trials have shown that these drugs are effective in reducing the risk of developing breast cancer. Talk with your doctor about whether an AI might be right for you. AIs can be used as an alternative to tamoxifen for women who have a higher risk of breast cancer and who have been through menopause. AIs are not used to treat women who have not been through menopause and are not usually recommended for those with osteoporosis.
The side effects of AIs may include hot flashes, fatigue, difficulty sleeping, diarrhea, joint and muscle pain, vaginal dryness, and bone loss.
This information is based on recommendations from the American Society of Clinical Oncology (ASCO) for the Use of Endocrine Therapy for Breast Cancer Risk Reduction . Please note that this link takes you to another ASCO website.
The next section in this guide is Screening . It explains how tests may find early breast cancer before signs or symptoms appear. Use the menu to choose a different section to read in this guide.
Breast Cancer - Screening
ON THIS PAGE: You will find out more about screening for breast cancer. You will also learn the risks and benefits of screening. Use the menu to see other pages.
Screening is used to look for cancer before you have any symptoms or signs. Scientists have developed, and continue to develop, tests that can be used to screen a person for specific types of cancer. The overall goals of breast cancer screening are to:
-
Detect the cancer at an earlier stage of disease, which is when the cancer is most curable
-
Lower the number of people who die from the disease, or eliminate deaths from cancer altogether
-
Identify people with a higher risk of developing a specific type of cancer who may need screening more often or a different type of screening due to genetic mutations or diseases
Learn more about the basics of cancer screening .
Screening information for breast cancer
Mammography
Mammography is the best tool doctors have to screen healthy people for breast cancer, as it has been shown to lower deaths from the disease. Like any medical test, mammography involves risks, such as the possibility of additional testing and anxiety if the test falsely shows a suspicious finding, called a "false-positive" result. Up to 10% to 15% of the time, mammography will not show an existing cancer, called a "false-negative" result.
Digital mammography may be better able to find breast cancers, particularly in dense breasts. A newer type of mammogram is called tomosynthesis or 3D mammography. It may improve the ability to find small cancers and reduce the need to repeat tests due to false-positives. However, there is also the risk of diagnosing problems in the breast that would otherwise go unnoticed and would not lead to any negative consequences. This is called "overdiagnosis" and may lead to overtreatment with a potential for harm. This method is approved by the U.S. Food and Drug Administration (FDA), though research on it is ongoing.
Other breast cancer screening methods
Other ways to examine the breasts, such as an ultrasound and/or a magnetic resonance imaging (MRI) scan , are not regularly used to screen for breast cancer in many women at average risk. However, these tests may be helpful when there is a very high risk of breast cancer, those with dense breast tissue, or when a lump or mass is found during a breast examination. The use of ultrasound screening is controversial because it has a high false-positive rate. This means that the test often wrongly identifies potential cancers. However, ultrasounds can be very useful in diagnosing breast cancer when an abnormality is found on mammogram (see Diagnosis ). MRI use in routine screening is also controversial, although there are very high-risk populations in which it is recommended.
According to the American Cancer Society (ACS), women who have BRCA gene mutations, who have a very strong family history of breast cancer, or who had prior radiation therapy to the chest should consider mammography and MRI each year.
Women at moderate risk of breast cancer, such as women with precancerous changes on a biopsy or mutations in other genes that increase risk of breast cancer, can talk with their doctor about whether MRI screening should be considered.
MRI may be better than mammography and ultrasound at finding a small mass in the breast, especially when there is very dense breast tissue. However, an MRI has a higher rate of false-positive test results, which may mean more biopsies, surgeries, and other tests that may lead to overdiagnosis. In addition, an MRI does not show small spots of calcium called calcifications that can be found on a mammogram. Calcifications can be a sign of non-invasive breast cancer (ductal carcinoma in situ, or DCIS). However, MRI can still be used to detect DCIS.
Ultrasound and/or MRI may also be used for a suspicious breast finding on physical examination or mammography. Studies have shown mammography combined with whole breast ultrasound may find slightly more breast cancers than mammography alone in women with dense breasts. If a lump or mass is found during a physical examination, further testing with ultrasound or mammography may be needed.
Sometimes, a mammogram and sonogram are staggered with an MRI 6 months apart as part of screening surveillance.
Talk with your doctor about the method of screening recommended for you and how often screening is needed.
Screening recommendations
Different organizations have looked at the evidence, risks, and benefits of mammography and have developed different screening recommendations. Decisions about screening for breast cancer are becoming increasingly individual. It is important to talk with your doctor about how often you should receive screening and which tests are most appropriate.
-
The U.S. Preventive Services Task Force (USPSTF) recommends that women ages 50 to 74 have mammography every 2 years. They recommend that mammography be considered in women ages 40 to 49 after evaluating the risks and benefits of this test with a doctor.
-
ACS recommends that women ages 40 to 44 have the choice to start yearly mammography. They recommend that women ages 45 to 54 receive mammography every year and that women 55 and older can switch to having a mammogram every 2 years or continue yearly screening if they choose or as long as they are in good health.
Other groups also provide recommendations regarding screening, including the American College of Radiology and the Society of Breast Imaging. Both recommend annual mammography starting at age 40. Some international groups do not recommend routine population-based screening for any age, but instead recommend an individualized approach.
The controversy about screening mammography is related to the risks versus the benefits associated with it. The benefit of this screening is finding a cancer early that could result in a better chance of a cure. The risk is a finding that leads to additional tests when cancer isn't present and how much harm those additional tests have on the patient. In many parts of the world, the controversy around screening mammography is also about feasibility and costs. Breast cancers detected by mammography are often small. In contrast, rapidly growing, aggressive cancers are more commonly found in between screening mammograms. They are called interval cancers. Interval cancers are more aggressive than screen-detected cancers and lead to more deaths compared to screen-detected cancers. They are also more frequently found in younger women.
If you have a higher risk of developing breast cancer, screening may be recommended at an earlier age and more often than the schedules listed above. Some older women may stop screening at some point , especially if they have significant health problems that limit the length of their life or ability to go through the physical demands of breast cancer treatment.
There are also different screening recommendations by groups for breast cancer survivors. Guidelines published in JAMA Oncology recommend that mammography be stopped for breast cancer survivors age 75 and older if they are expected to live less than 5 years. Meanwhile, they recommend that mammography be continued for breast cancer survivors age 75 and older who are expected to live more than 10 years.
This is why it is important to talk with your doctor about breast cancer screening and decide on an appropriate screening schedule for you.
The USPSTF and ACS also differ on their recommendations for clinical breast examinations. A clinical breast examination is when a doctor or other health care professional performs a physical examination of your breasts to check for abnormalities or lumps. The USPSTF recommends a clinical breast examination along with mammography. The ACS does not recommend a clinical breast examination for women with an average risk of developing breast cancer, as they say there is very little evidence that it helps find breast cancer early when women are also getting mammograms. However, the ACS notes that this does not mean these examinations should never be done.
Finally, although breast self-examination has not been shown to lower deaths from breast cancer, it is important to become familiar with your breasts so that you can be aware of any changes and report these to the doctor. Cancers that are growing more quickly are often found through breast examinations in between regular mammograms.
The next section in this guide is Symptoms and Signs . It explains what changes or medical problems breast cancer can cause. Use the menu to choose a different section to read in this guide.
Breast Cancer - Symptoms and Signs
ON THIS PAGE: You will find out more about changes and other things that can signal a problem that may need medical care. Use the menu to see other pages.
Many people with breast cancer do not have any body changes (signs) or symptoms when they are first diagnosed with breast cancer. Symptoms are changes that you can feel in your body. Signs are changes in something measured, like by taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem. Many times, the cause of a symptom or sign may be a medical condition that is not cancer.
However, some people do have symptoms or signs when they are first diagnosed with breast cancer. If a person develops one or more of the following symptoms or signs, they should discuss them with a doctor.
-
A lump that feels like a hard knot or a thickening in the breast or under the arm. It is important to feel the same area in the other breast to make sure the change is not a part of healthy breast tissue in that area.
-
Change in the size or shape of the breast
-
Nipple discharge that occurs suddenly in a non-lactating person, is bloody, or occurs in only 1 breast
-
Physical changes, such as a nipple turned inward or a sore located in the nipple area
-
Skin irritation or changes, such as puckering, dimpling, scaliness, or new creases
-
A warm, red, swollen breast with or without a rash with dimpling resembling the skin of an orange, called “peau d'orange”
-
Pain in the breast, particularly breast pain that does not go away. Pain is not usually a symptom of breast cancer, but it should be reported to a doctor.
If you are concerned about any changes you experience, including those listed above as well as other concerning changes that are not, please talk with your doctor. Your doctor will ask how long and how often you have been experiencing the symptom(s), in addition to other questions. This is to help figure out the cause of the problem, called a diagnosis.
If cancer is diagnosed, relieving symptoms is an important part of cancer care and treatment. Managing symptoms may also be called "palliative care" or "supportive care." It is often started soon after diagnosis and continued throughout treatment. Be sure to talk with your health care team about the symptoms you experience, including any new symptoms or a change in symptoms.
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Breast Cancer - Diagnosis
ON THIS PAGE: You will find a list of common tests, procedures, and scans that doctors use to find the cause of a medical problem. Use the menu to see other pages.
Doctors use many tests to find, or diagnose, breast cancer. They may also do tests to learn if the cancer has spread to a part of the body other than the breast and the lymph nodes under the arm. If the cancer has spread, it is called metastasis (see the Metastatic Breast Cancer guide for more information). Doctors may also do tests to learn which treatments could work best.
For most types of cancer, a biopsy is the only sure way for the doctor to know if an area of the body has cancer. In a biopsy, the doctor takes a small sample of tissue for testing in a laboratory. If a biopsy is not possible, the doctor may suggest other tests that will help make a diagnosis.
How breast cancer is diagnosed
There are many tests used to diagnose breast cancer. Not all tests described here will be used for every person. Your doctor may consider these factors when choosing a diagnostic test:
-
The type of cancer suspected
-
Your signs and symptoms
-
Your age and general health
-
The results of earlier medical tests
The series of tests needed to evaluate a possible breast cancer usually begins when a person or their doctor discovers a mass or abnormal calcifications on a screening mammogram, or a lump or nodule in the breast during a clinical or self-examination. Less commonly, a person might notice a red or swollen breast or a mass or nodule under the arm.
The tests described below may be used to diagnose breast cancer or be used for follow-up testing after a breast cancer diagnosis is made.
Imaging tests
Imaging tests show pictures of the inside of the body. They can show if cancer has spread. The following imaging tests of the breast may be done to learn more about a suspicious area found in the breast during screening. In addition to these, there are other new types of tests that are being studied.
-
Diagnostic mammography. Diagnostic mammography is similar to screening mammography except that more pictures of the breast are taken. It is often used when a person is experiencing signs, such as a new lump or nipple discharge. Diagnostic mammography may also be used if something suspicious is found on a screening mammogram.
-
Ultrasound. An ultrasound uses sound waves to create a picture of the breast tissue. An ultrasound can distinguish between a solid mass, which may be cancer, and a fluid-filled cyst, which is usually not cancer. When ultrasound is used to examine a finding that could be cancer, it is often used to examine that specific area of the breast rather than the whole breast.
-
Magnetic resonance imaging (MRI). An MRI uses magnetic fields, not x-rays, to produce detailed images of the body. A special dye called a contrast medium is given before the scan to help create a clear picture of the possible cancer. This dye is injected into the patient’s vein. A breast MRI may be used after a person has been diagnosed with cancer to find out how much the disease has grown throughout the breast or to check the other breast for cancer. Breast MRI may also be a screening option, along with mammography, for someone with a very high risk of developing breast cancer and for some women who have a history of breast cancer (see Risk Factors and Prevention ). MRI may also be used if locally advanced breast cancer is diagnosed or if chemotherapy or hormonal therapy is being given first, followed by a repeated MRI for surgical planning (see Types of Treatment ). Finally, MRI may be used as a surveillance method following breast cancer diagnosis and treatment.
Biopsy
A biopsy is the removal of a small amount of tissue for examination under a microscope. Other tests can suggest that cancer is present, but only a biopsy can make a definite diagnosis. A pathologist then analyzes the sample(s). A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease. There are different types of biopsies, classified by the technique and/or size of needle used to collect the tissue sample.
-
Fine needle aspiration biopsy. This type of biopsy uses a thin needle to remove a small sample of cells.
-
Core needle biopsy. This type of biopsy uses a wider needle to remove a larger sample of tissue. This is usually the preferred biopsy technique. If a tumor is identified, the cancer biomarkers, such as hormone receptor status (ER, PR) and HER2 status, will be tested to help guide treatment options. These biomarkers are found on or in the tumor cells. Additional types of biomarkers that are made by the tumor or by the body in response to the cancer can be found in the blood or other fluids, although these are not commonly used to establish a breast cancer diagnosis. This information will help the doctor recommend a treatment plan. Local anesthesia, which is medication to block pain, is used to lessen the patient’s discomfort during the procedure.
-
Image-guided biopsy. During this procedure, a needle is guided to the location of the mass or calcifications with the help of an imaging technique, such as mammography, ultrasound, or MRI. These are usually core needle biopsies, but they can also be fine needle aspiration biopsies. A stereotactic biopsy is a type of image-guided biopsy that is done using mammography to help guide the needle. Your doctor will let you know what type of biopsy is best for your situation. A small metal clip is usually put into the breast at the time of biopsy to mark where the biopsy sample was taken, in case the tissue is cancerous and more surgery is needed. This clip is usually titanium, so it will not cause problems with future imaging tests, but check with your doctor before you have any imaging tests done.
-
Surgical biopsy. This type of biopsy removes the largest amount of tissue. Because surgery is best done after a cancer diagnosis has been made, a surgical biopsy is usually not the recommended way to diagnose breast cancer. Most often, non-surgical core needle biopsies are recommended to diagnose breast cancer in order to limit the amount of tissue removed. Since many people who are recommended to undergo breast biopsy are not diagnosed with cancer, using a needle biopsy for diagnosis reduces the number of people who have surgery unnecessarily.
-
Sentinel lymph node biopsy. When cancer spreads through the lymphatic system, the lymph node or group of lymph nodes the cancer reaches first is called the “sentinel” lymph node. In breast cancer, these are usually the lymph nodes under the arms called the axillary lymph nodes. The sentinel lymph node biopsy procedure is a way to find out if there is cancer in the lymph nodes near the breast. Learn more about sentinel lymph node biopsy in the Types of Treatment section.
Analyzing the biopsy sample
Analyzing the sample(s) removed during the biopsy can help your doctor learn about specific features of a cancer that help determine your treatment options.
-
Tumor features. Examination of the tumor under the microscope is used to determine if it is invasive or non-invasive (in situ); ductal, lobular, or another type of breast cancer; and whether the cancer has spread to the lymph nodes. The margins or edges of the tumor are also examined, and the distance from the tumor to the edge of the tissue that was removed is measured, which is called margin width.
-
Estrogen receptors (ER) and progesterone receptors (PR). Testing for ER and PR (see Introduction ) helps determine both the patient’s risk of recurrence (risk of the cancer coming back) and the type of treatment that is most likely to lower the risk of recurrence. Generally, hormonal therapy, also called endocrine therapy or hormone-blocking therapy (see Types of Treatment ), reduces the chance of recurrence of ER-positive and/or PR-positive cancers. Guidelines from ASCO and the College of American Pathologists recommend that the ER and PR status should be tested on the breast tumor and/or areas of spread for everyone newly diagnosed with invasive breast cancer or when there is a breast cancer recurrence. For those with ductal carcinoma in situ (DCIS), testing for ER status is recommended to find out if hormone therapy may reduce the risk of future breast cancer.
-
Human epidermal growth factor receptor 2 (HER2). The HER2 status of the cancer (see Introduction ) helps determine whether drugs that target the HER2 receptor, such as trastuzumab (Herceptin) and pertuzumab (Perjeta), might help treat the cancer. This test is only done on invasive cancers. Guidelines recommend that HER2 testing be done when you are first diagnosed with an invasive breast cancer. In addition, if the cancer has spread to another part of your body or comes back after treatment, testing should be done again on the new tumor or areas where the cancer has spread.
In early-stage breast cancer, HER2 tests are usually clearly positive or negative, meaning that your cancer has either a high level or a low or absent level of HER2. If your test results are not clearly positive or negative, additional testing may need to be done, either on a different tumor sample or with a different test. Sometimes, even with repeated testing, the results may not be conclusive, so you and your doctor will have to discuss the best treatment option.
If the cancer is HER2 positive, HER2-targeted therapy may be a recommended treatment option for you.
-
Grade. The tumor grade is also determined from a biopsy. Grade refers to how different the cancer cells look from healthy cells and whether they appear slower growing or faster growing. If the cancer looks similar to healthy tissue and has different cell groupings, it is called "well differentiated" or a "low-grade tumor." If the cancerous tissue looks very different from healthy tissue, it is called "poorly differentiated" or a "high-grade tumor." There are 3 grades: grade 1 (well differentiated), grade 2 (moderately differentiated), and grade 3 (poorly differentiated).
Results of these tests can help determine your treatment options , which are outlined in another section in this guide.
Genomic tests to predict recurrence risk
Doctors use genomic tests, also called multigene panels, to test a tumor to look for specific genes or proteins that are found in or on cancer cells. These tests help doctors better understand the unique features of a person's breast cancer. Genomic tests can also help estimate the risk of the cancer coming back after treatment. Knowing this information helps doctors and patients make decisions about specific treatments and can help some patients avoid unwanted side effects from a treatment they may not need.
Genomic tests are different from genetic tests. Genetic tests are performed on blood or saliva and are used to determine what gene changes a person may have inherited from a parent that may increase their risk of developing breast cancer. The results of a few genetic tests (for example, tests looking for BRCA1 and BRCA2 ) can also be used to make decisions about specific treatments.
The genomic tests listed below can be done on a sample of the tumor that was already removed during biopsy or surgery. Most patients will not need an extra biopsy or more surgery for these tests.
-
Oncotype Dx™ . This test is an option for people with ER-positive and/or PR-positive, HER2-negative breast cancer that has not spread to the lymph nodes. It is also an option in some cases where the cancer has spread to 1 to 3 lymph nodes, such as for women who have been through menopause. This test can help patients and their doctors make decisions about whether chemotherapy should be added to hormonal therapy. This test looks at 16 cancer-related genes and 5 reference genes to calculate a “recurrence score” that estimates the risk of the cancer coming back outside of the breast or regional lymph nodes within 10 years after diagnosis, assuming a patient takes 5 years of hormonal therapy. The recurrence score is used to guide recommendations on the use of chemotherapy. For example, the American Society of Clinical Oncology (ASCO) recommends that people with a recurrence score of 26 or higher should be offered chemotherapy followed by hormonal therapy. Recommendations are listed by age group below. Oncotype Dx™ testing is not recommended for people whose cancer has spread to the lymph nodes if they have not yet been through menopause. It is important to talk with your doctor about the specific testing and treatment recommendation for you.
For patients age 50 or younger who do not have cancer in any lymph nodes
-
Recurrence score less than 16: Hormonal therapy is usually recommended, but chemotherapy is generally not needed
-
Recurrence score of 16 to 25: Chemotherapy may be recommended before hormonal therapy is given
-
Recurrence score of 26 or higher: Chemotherapy is usually recommended before hormonal therapy is given
For patients age 50 or younger who have cancer in 1 to 3 lymph nodes
-
Recurrence score less than 26: Chemotherapy is often recommended before hormonal therapy is given
-
Recurrence score of 26 or higher: Chemotherapy is usually recommended before hormonal therapy is given
For patients older than 50 who do not have cancer in any lymph nodes or who have cancer in 1 to 3 lymph nodes
-
Recurrence score less than 26: Hormonal therapy is usually recommended, but chemotherapy is generally not needed
-
Recurrence score of 26 or higher: Chemotherapy is usually recommended before hormonal therapy is given
-
-
MammaPrint™ . This test is an option for people older than 50 with ER-positive and/or PR-positive, HER2-negative breast cancer that has spread to 3 or fewer lymph nodes. This test uses information from 70 genes to estimate the risk of recurrence for early-stage breast cancer. For people with a high risk of the cancer coming back based on the size and grade of the cancer, this test can help patients and their doctors make decisions about whether chemotherapy should be given before hormonal therapy. This test is not recommended for people with a low risk of the cancer coming back, for people 50 or younger, or for people with cancer in more than 3 lymph nodes.
-
EndoPredict . This test is an option for people with ER-positive, HER2-negative breast cancer that has spread to 3 or fewer lymph nodes and who have been through menopause. This test uses information from 12 genes to estimate the risk of the cancer coming back within 10 years after diagnosis. This test can help patients and their doctors make decisions about whether chemotherapy and hormonal therapy should be given following surgery.
-
Prosigna™ (PAM50). This test is an option for people who have been through menopause and have ER-positive, HER2-negative breast cancer that has not spread to the lymph nodes. This test uses information from 50 genes to estimate the risk of the cancer coming back within 10 years after diagnosis. This test can help patients and their doctors make decisions about whether chemotherapy and hormonal therapy should be given following surgery.
-
Additional tests. There are additional tests that may be options for people with ER-positive and/or PR-positive, HER2-negative breast cancer that has not spread to the lymph nodes or has spread to 1 to 3 lymph nodes. They can also be used to estimate how likely it is that the cancer will spread to other parts of the body.
-
Ki-67 index. Ki-67 is a protein in cells that increases as they prepare to divide. If there is a high percentage of cells with the Ki-67 protein in the tumor, it means that the cells are dividing rapidly. The Ki-67 index, which is also called a proliferative index, is an indicator of how quickly the tumor cells are multiplying. When the genomic tests described above cannot be used for people with stage I or II breast cancer who have been through menopause, the Ki-67 index may be used to help patients and their doctors make decisions about whether chemotherapy and hormonal therapy should be given following surgery.
-
Immunohistochemistry 4 (IHC). This test uses ER, PR, and HER2 status as well as the Ki-67 index from a sample of tumor to estimate the risk of the cancer coming back within 10 years after diagnosis. It can be used for people whose cancer has not spread to the lymph nodes or has only spread to 1 to 3 lymph nodes and when the genomic tests described above are not available. This test can help patients and their doctors make decisions about whether chemotherapy should be given before hormonal therapy.
-
Breast Cancer Index (BCI). This test uses information from 11 genes to estimate the risk of the cancer coming back within 5 to 10 years after a diagnosis. It is used for people whose cancer has not spread to the lymph nodes or has only spread to 1 to 3 lymph nodes. For a patient who has had 5 years of hormonal therapy and who has no evidence of cancer recurrence, this test can help patients and their doctors make decisions about whether additional hormonal therapy with tamoxifen, an AI, or tamoxifen followed by an AI is needed (see Types of Treatment ).
-
Clinical Treatment Score post-5 years (CTS5). This is an online tool doctors can use to calculate the risk of cancer recurrence between 5 and 10 years after a diagnosis. ASCO recommends using CTS5 for people who have been through menopause, have received 5 years of hormonal therapy for invasive breast cancer, and have not had a recurrence. This tool can help patients and their doctors make decisions about whether additional hormonal therapy may be needed.
-
The tests described above have not been shown to be useful to predict risk of recurrence for people with HER2-positive or triple-negative breast cancer. Therefore, none of these tests are currently recommended for testing HER2-positive or triple-negative breast cancer. They are also not recommended for people who have cancer in more than 3 lymph nodes. Your doctor will use other factors to help recommend treatment options for you.
Talk with your doctor for more information about genomic tests, what they mean, and how the results might affect your treatment plan.
This information is based on several ASCO recommendations, including the Use of Biomarkers to Guide Decisions on Adjuvant Systemic Therapy for Women with Early-Stage Invasive Breast Cancer , Biomarkers for Adjuvant Endocrine and Chemotherapy in Early-Stage Breast Cancer , and ASCO’s endorsement of recommendations from Cancer Care Ontario on the Role of Patient and Disease Factors in Adjuvant Systemic Therapy Decision-Making for Early-Stage, Operable Breast Cancer . Please note that these links take you to another ASCO website.
Blood tests
Your doctor may also need to do several types of blood tests. These tests may be done before or after surgery.
-
Complete blood count. A complete blood count (CBC) is used to measure the number of different types of cells, such as red blood cells and white blood cells, in a sample of a person’s blood. It is done to make sure that your bone marrow is functioning well.
-
Blood chemistry. This test evaluates how well your liver and kidneys are working.
-
Hepatitis tests. These tests are used to check for evidence of prior exposure to hepatitis B and/or hepatitis C. If you have evidence of an active hepatitis B infection, you may need to take a special medication to suppress the virus before you receive chemotherapy. Without this medication, the chemotherapy can cause the virus to grow and damage the liver. Learn more about hepatitis B screening before treatment .
After diagnostic tests are completed, your doctor will review the results with you. If the diagnosis is cancer, these results also help the doctor describe the cancer. This is called staging. Depending on the stage of the cancer and the tumor biomarkers, additional imaging tests may be recommended. If there is a suspicious area found outside of the breast and nearby lymph nodes, you may need a biopsy of other parts of the body to find out if it is cancer.
The next section in this guide is Stages . It explains the system doctors use to describe the extent of the disease. Use the menu to choose a different section to read in this guide.
Breast Cancer - Stages
ON THIS PAGE: You will learn about how doctors describe a cancer’s growth or spread. This is called the stage. Use the menu to see other pages.
What is cancer staging?
Staging is a way of describing how extensive the breast cancer is, including the size of the tumor, whether it has spread to lymph nodes, whether it has spread to distant parts of the body, and what its biomarkers are.
Staging can be done either before or after a patient undergoes surgery. Staging done before surgery is called the clinical stage, and staging done after surgery is called the pathologic stage. Doctors use diagnostic tests to find out the cancer's stage, so staging may not be complete until all of the tests are finished. Knowing the stage helps the doctor recommend the best kind of treatment and can help predict a patient's prognosis, which is the chance of recovery. There are different stage descriptions for different types of cancer.
This page provides detailed information about the system used to find the stage of breast cancer and the stage groups for breast cancer.
-
TNM staging system
-
Stage groups for breast cancer
TNM staging system
The most common tool that doctors use to describe the stage is the TNM system. Doctors use the results from diagnostic tests and scans to answer these questions:
-
Tumor (T): How large is the primary tumor in the breast? What are its biomarkers?
-
Node (N): Has the tumor spread to the lymph nodes? If so, where, what size, and how many?
-
Metastasis (M): Has the cancer spread to other parts of the body?
The results are combined to determine the stage of cancer for each person.
There are 5 major stages of breast cancer: stage 0 (zero), which is non-invasive ductal carcinoma in situ (DCIS), and stages I through IV (1 through 4), which are used for invasive breast cancer. The stage provides a common way of describing the cancer, so doctors can work together to plan the best treatments.
Staging can be clinical and/or pathological. Clinical staging is based on the results of tests done before surgery, which may include physical examinations, mammogram, ultrasound, and MRI scans. Pathological staging is based on what is found during surgery to remove breast tissue and lymph nodes. The results are usually available several days after surgery. In general, pathological staging provides the most information to determine a patient’s prognosis.
Here are more details on each part of the TNM system for breast cancer:
Tumor (T)
Using the TNM system, the “T” plus a letter or number (0 to 4) is used to describe the size and location of the tumor. Tumor size is measured in centimeters (cm). A centimeter is roughly equal to the width of a standard pen or pencil.
Stage may also be divided into smaller groups that help describe the tumor in even more detail. Specific tumor stage information in listed below.
TX:
The primary tumor cannot be evaluated.
T0 (T zero):
There is no evidence of cancer in the breast.
Tis: Refers to carcinoma in situ . The cancer is confined within the ducts of the breast tissue and has not spread into the surrounding tissue of the breast. There are 2 types of breast carcinoma in situ:
-
Tis (DCIS): DCIS is a non-invasive cancer, but if not removed, it may develop into an invasive breast cancer later. DCIS means that cancer cells have been found in breast ducts and have not spread past the layer of tissue where they began.
-
Tis (Paget’s disease): Paget's disease of the nipple is a rare form of early, non-invasive cancer that is only in the skin cells of the nipple. Sometimes Paget's disease is associated with an invasive breast cancer. If there is an invasive breast cancer, it is classified according to the stage of the invasive tumor.
T1: The tumor in the breast is 20 millimeters (mm) or smaller in size at its widest area. This is a little less than an inch. This stage is then broken into 4 substages depending on the size of the tumor:
-
T1mi is a tumor that is 1 mm or smaller.
-
T1a is a tumor that is larger than 1 mm but 5 mm or smaller.
-
T1b is a tumor that is larger than 5 mm but 10 mm or smaller.
-
T1c is a tumor that is larger than 10 mm but 20 mm or smaller.
T2: The tumor is larger than 20 mm but not larger than 50 mm.
T3:
The tumor is larger than 50 mm.
T4:
The tumor falls into 1 of the following groups:
-
T4a means the tumor has grown into the chest wall.
-
T4b is when the tumor has grown into the skin.
-
T4c is cancer that has grown into the chest wall and the skin.
-
T4d is inflammatory breast cancer .
Node (N)
The “N” in the TNM staging system stands for lymph nodes. These small, bean-shaped organs help fight infection. Lymph nodes near where the cancer started are called regional lymph nodes. Regional lymph nodes include:
-
Lymph nodes located under the arm, called the axillary lymph nodes
-
Lymph nodes located above and below the collarbone
-
Lymph nodes located under the breastbone, called the internal mammary lymph nodes
Lymph nodes in other parts of the body are called distant lymph nodes. The information below describes the staging.
NX:
The lymph nodes were not evaluated.
N0: Either of the following:
-
No cancer was found in the lymph nodes.
-
Only areas of cancer smaller than 0.2 mm are in the lymph nodes.
N1: The cancer has spread to 1 to 3 axillary lymph nodes and/or the internal mammary lymph nodes. If the cancer in the lymph node is larger than 0.2 mm but 2 mm or smaller, it is called "micrometastatic" (N1mi).
N2: The cancer has spread to 4 to 9 axillary lymph nodes. Or, it has spread to the internal mammary lymph nodes, but not the axillary lymph nodes.
N3: The cancer has spread to 10 or more axillary lymph nodes, or it has spread to the lymph nodes located under the clavicle, or collarbone. It may have also spread to the internal mammary lymph nodes. Cancer that has spread to the lymph nodes above the clavicle, called the supraclavicular lymph nodes, is also described as N3.
If there is cancer in the lymph nodes, knowing how many lymph nodes are involved and where they are helps doctors to plan treatment. The pathologist can find out the number of axillary lymph nodes that contain cancer after they are removed during surgery. It is not common to remove the supraclavicular or internal mammary lymph nodes during surgery. If there is cancer in these lymph nodes, treatment other than surgery, such as radiation therapy, chemotherapy, and hormonal therapy, is generally used.
Metastasis (M)
The “M” in the TNM system describes whether the cancer has spread to other parts of the body, called metastasis. This is no longer considered early-stage or locally advanced cancer. For more information, see this website's
Guide to Metastatic Breast Cancer
.
MX:
Distant spread cannot be evaluated.
M0: There is no evidence of distant metastases.
M0 (i+): There is no clinical or radiographic evidence of distant metastases. However, there is microscopic evidence of tumor cells in the blood, bone marrow, or other lymph nodes that are no larger than 0.2 mm.
M1: There is evidence of metastasis to another part of the body, meaning there are breast cancer cells growing in other organs.
Return to top
Stage groups for breast cancer
Doctors assign the stage of the cancer by combining the T, N, and M classifications (see above), the tumor grade, and the results of ER/PR and HER2 testing. This information is used to help determine your prognosis (see Diagnosis ). The simpler approach to explaining the stage of breast cancer is to use the T, N, and M classifications alone. This is the approach used below to describe the different stages.
Most patients are anxious to learn the exact stage of the cancer. If you have surgery as the first treatment for your cancer, your doctor will generally confirm the stage of the cancer when the testing after surgery is finalized, usually about 5 to 7 days after surgery. When systemic treatment (see
Types of Treatment
) is given before surgery, which is typically with medications and is called neoadjuvant therapy, the stage of the cancer is primarily determined clinically. Doctors may refer to stage I to stage IIA cancer as "early stage" and stage IIB to stage III as "locally advanced."
Stage 0:
Stage zero (0) describes disease that is only in the ducts of the breast tissue and has not spread to the surrounding tissue of the breast. It is also called non-invasive or in situ cancer (Tis, N0, M0).
Stage IA:
The tumor is small, invasive, and has not spread to the lymph nodes (T1, N0, M0).
Stage IB:
Cancer has spread to the lymph nodes and the cancer in the lymph node is larger than 0.2 mm but less than 2 mm in size. There is either no evidence of a tumor in the breast or the tumor in the breast is 20 mm or smaller (T0 or T1, N1mi, M0).
Stage IIA: Any 1 of these conditions:
-
There is no evidence of a tumor in the breast, but the cancer has spread to 1 to 3 axillary lymph nodes. It has not spread to distant parts of the body (T0, N1, M0).
-
The tumor is 20 mm or smaller and has spread to 1 to 3 axillary lymph nodes (T1, N1, M0).
-
The tumor is larger than 20 mm but not larger than 50 mm and has not spread to the axillary lymph nodes (T2, N0, M0).
Stage IIB: Either of these conditions:
-
The tumor is larger than 20 mm but not larger than 50 mm and has spread to 1 to 3 axillary lymph nodes (T2, N1, M0).
-
The tumor is larger than 50 mm but has not spread to the axillary lymph nodes (T3, N0, M0).
Stage IIIA: The tumor of any size has spread to 4 to 9 axillary lymph nodes or to internal mammary lymph nodes. It has not spread to other parts of the body (T0, T1, T2, or T3; N2; M0). Stage IIIA may also be a tumor larger than 50 mm that has spread to 1 to 3 axillary lymph nodes (T3, N1, M0).
Stage IIIB:
The tumor has spread to the chest wall or caused swelling or ulceration of the breast, or it is diagnosed as
inflammatory breast cancer
. It may or may not have spread to up to 9 axillary or internal mammary lymph nodes. It has not spread to other parts of the body (T4; N0, N1, or N2; M0).
Stage IIIC:
A tumor of any size that has spread to 10 or more axillary lymph nodes, the internal mammary lymph nodes, and/or the lymph nodes under the collarbone. It has not spread to other parts of the body (any T, N3, M0).
Stage IV (metastatic): The tumor can be any size and has spread to other organs, such as the bones, lungs, brain, liver, distant lymph nodes, or chest wall (any T, any N, M1). Metastatic breast cancer that is found when the cancer is first diagnosed occurs about 6% of the time. This may be called de novo metastatic breast cancer. Most commonly, metastatic breast cancer is found after a previous diagnosis and treatment of early stage breast cancer. Learn more about metastatic breast cancer .
Recurrent: Recurrent cancer is cancer that has come back after treatment and can be described as local, regional, and/or distant. If the cancer does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis .
Return to top
Used with permission of the American College of Surgeons, Chicago, Illinois. The original and primary source for this information is the
AJCC Cancer Staging Manual, Eighth Edition (2017)
, published by Springer International Publishing.
Information about the cancer’s stage will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment . Use the menu to choose a different section to read in this guide.
Breast Cancer - Types of Treatment
ON THIS PAGE: You will learn about the different types of treatments doctors use for people with breast cancer. Use the menu to see other pages.
This section explains the types of treatments, also known as therapies, that are the standard of care for early-stage and locally advanced breast cancer. “Standard of care” means the best treatments known. When making treatment plan decisions, you are encouraged to discuss with your doctor whether clinical trials are an option. A clinical trial is a research study that tests a new approach to treatment. Doctors learn through clinical trials whether a new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug and how often it should be given, a new combination of standard treatments, or new doses of standard drugs or other treatments. Some clinical trials also test giving less drug or radiation treatment or doing less extensive surgery than what is usually done as the standard of care. Clinical trials are an option for all stages of cancer. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
How breast cancer is treated
In cancer care, doctors specializing in different areas of cancer treatment—such as surgery, radiation oncology, and medical oncology—work together with radiologists and pathologists to create a patient’s overall treatment plan that combines different types of treatments. This is called a multidisciplinary team . Cancer care teams include a variety of other health care professionals, such as physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, genetic counselors, nutritionists, therapists, and others. For people older than 65, a geriatric oncologist or geriatrician may also be involved in their care. Ask the members of your treatment team who is the primary contact for questions about scheduling and treatment, who is in charge during different parts of treatment, how they communicate across teams, and whether there is 1 contact who can help with communication across specialties, such as a nurse navigator. This can change over time as your health care needs change.
A treatment plan is a summary of your cancer and the planned cancer treatment. It is meant to give basic information about your medical history to any doctors who will care for you during your lifetime. Before treatment begins, ask your doctor for a copy of your treatment plan. You can also provide your doctor with a copy of the ASCO Treatment Plan form to fill out.
The biology and behavior of breast cancer affects the treatment plan. Some tumors are smaller but grow quickly, while others are larger and grow slowly. Treatment options and recommendations are very personalized and depend on several factors, including:
-
The tumor’s subtype, including hormone receptor status (ER, PR), HER2 status, and nodal status (see Introduction )
-
The stage of the tumor
-
Genomic tests, such as the multigene panels Oncotype DX™ or MammaPrint™, if appropriate (See Diagnosis )
-
The patient’s age, general health, menopausal status, and preferences
-
The presence of known mutations in inherited breast cancer genes, such as BRCA1 or BRCA2, based on results of genetic tests
Even though the breast cancer care team will specifically tailor the treatment for each patient and tumor, called "personalized medicine," there are some general steps for treating early-stage and locally advanced breast cancer.
For both ductal carcinoma in situ (DCIS) and early-stage invasive breast cancer, doctors generally recommend surgery to remove the tumor. To make sure that the entire tumor is removed, the surgeon will also remove a small area of healthy tissue around the tumor, called a margin. Although the goal of surgery is to remove all of the visible cancer in the breast, microscopic cells can be left behind. In some situations, this means that another surgery could be needed to remove remaining cancer cells. There are different ways to check for microscopic cells that will ensure a clean margin. It is also possible for microscopic cells to be present outside of the breast, which is why systemic treatment with medication is often recommended after surgery, as described below.
For larger cancers, or those that are growing more quickly, doctors may recommend systemic treatment with chemotherapy, immunotherapy, and/or hormonal therapy before surgery, called neoadjuvant therapy. There may be several benefits to having drug treatments before surgery:
-
Surgery may be easier to perform because the tumor is smaller.
-
Your doctor may find out if certain treatments work well for the cancer.
-
You may be able to try a new treatment through a clinical trial.
-
If you have any microscopic distant disease, it will be treated earlier by the drug therapy that circulates through the body.
-
People who may have needed a mastectomy could have breast-conserving surgery (lumpectomy) if the tumor shrinks enough before surgery.
After surgery, the next step in managing early-stage breast cancer is to lower the risk of recurrence and to try to get rid of any remaining cancer cells in the body. These cancer cells are undetectable with current tests but are believed to be responsible for a cancer recurrence, as they can grow over time. Treatment given after surgery is called "adjuvant therapy." Adjuvant therapies may include radiation therapy, chemotherapy, targeted therapy, immunotherapy, and/or hormonal therapy (see below for more information on each of these treatments).
Whether adjuvant therapy is needed depends on the chance that any cancer cells remain in the breast or the body and the chance that a specific treatment will work to treat the cancer. Although adjuvant therapy lowers the risk of recurrence, it does not completely get rid of the risk.
Along with staging, other tools can help estimate prognosis and help you and your doctor make decisions about adjuvant therapy. Depending on the subtype of breast cancer, this includes tests that can predict the risk of recurrence by testing your tumor tissue (such as Oncotype Dx™ or MammaPrint™; see Diagnosis ). Such tests may also help your doctor better understand whether chemotherapy will help reduce the risk of recurrence.
If surgery to remove the cancer is not possible, it is called inoperable. The doctor will then recommend treating the cancer in other ways. Chemotherapy, immunotherapy, targeted therapy, radiation therapy, and/or hormonal therapy may be given to shrink the cancer.
For recurrent cancer, treatment options depend on how the cancer was first treated and the characteristics of the cancer mentioned above, such as ER, PR, and HER2.
Take time to learn about all of your treatment options and be sure to ask questions about things that are unclear. Talk with your doctor about the goals of each treatment and what you can expect while receiving the treatment. These types of talks are called “shared decision-making.” Shared decision-making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision-making is particularly important for people with breast cancer because there are different treatment options. It is also important to check with your health insurance company before any treatment begins to make sure the planned treatment is covered.
People older than 65 may benefit from having a geriatric assessment before planning treatment. Find out what a geriatric assessment involves and how it can help people older than 65 with cancer .
Learn more about making treatment decisions .
The common types of treatments used for early-stage and locally advanced breast cancer are described below. Your care plan also includes treatment for symptoms and side effects, which is an important part of cancer care.
-
Surgery
-
Radiation therapy
-
Chemotherapy
-
Hormonal therapy
-
Targeted therapy
-
Immunotherapy
-
Neoadjuvant systemic therapy for non-metastatic breast cancer
-
Systemic therapy concerns for people age 65 or older
-
Physical, emotional, and social effects of cancer
-
Recurrent breast cancer
Surgery
Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. Surgery is also used to examine the nearby axillary lymph nodes, which are under the arm. A surgical oncologist is a doctor who specializes in treating cancer with surgery. Learn more about the basics of cancer surgery .
The choice of surgery does not affect whether you will need therapy using medication, such as chemotherapy, hormone therapy, and/or targeted therapy (see below). Drug therapies are given based on the characteristics of the tumor, not the type of surgery you have.
Generally, the smaller the tumor, the more surgical options a patient has . The types of surgery for breast cancer include the following:
-
Lumpectomy. This is the removal of the tumor and a small, cancer-free margin of healthy tissue around the tumor. Most of the breast remains. For invasive cancer, radiation therapy to the remaining breast tissue is often recommended after surgery, especially for younger patients, patients with hormone receptor-negative tumors, and patients with larger tumors. For DCIS, radiation therapy after surgery is usually given. A lumpectomy may also be called breast-conserving surgery, a partial mastectomy, a quadrantectomy, or a segmental mastectomy.
-
Mastectomy. This is the surgical removal of the entire breast. There are several types of mastectomies. Talk with your doctor about whether the skin can be preserved, called a skin-sparing mastectomy, or whether the nipple can be preserved, called a nipple-sparing mastectomy or total skin-sparing mastectomy. Your doctor will also consider how large the tumor is compared to the size of your breast in determining the best type of surgery for you. Radiation therapy may be recommended following mastectomy. Learn more about the different types of mastectomies and exercising after a mastectomy.
Lymph node removal, analysis, and treatment
Cancer cells can be found in the axillary lymph nodes in some cancers. Knowing whether any of the lymph nodes near the breast contain cancer can provide useful information to determine treatment and prognosis.
-
Sentinel lymph node biopsy.
In a sentinel lymph node biopsy (also called a sentinel node biopsy or SNB), the surgeon finds and removes 1 to 3 or more lymph nodes from under the arm that receive lymph drainage from the breast. This procedure is generally not an option when the doctor already knows based on clinical evaluation that the lymph nodes have cancer. Rather, it may be an option for patients with no obvious clinical evidence of lymph node involvement. This procedure helps avoid removing a larger number of lymph nodes with an axillary lymph node dissection (see below) for patients whose sentinel lymph nodes are mostly free of cancer. The smaller lymph node procedure helps lower the risk of several possible side effects. Those side effects include swelling of the arm called
lymphedema
, numbness, and arm movement and range of motion problems with the shoulder. These can be long-lasting issues that can severely affect a person’s quality of life. Importantly, the risk of lymphedema increases with the number of lymph nodes and lymph vessels that are removed or damaged during cancer treatment. This means that people who have a sentinel lymph node biopsy are less likely to develop lymphedema than those who have an axillary lymph node dissection (see below).
Your doctor may recommend imaging of your lymph nodes with an ultrasound and/or an image-guided biopsy of the lymph nodes before a sentinel lymph node biopsy to find out if the cancer has spread there (see Diagnosis ). This is often done if you have a large cancer, if your lymph nodes can be felt during clinical examination, or if you are having treatment with chemotherapy before surgery. However, the American Society of Clinical Oncology (ASCO) does not recommend doing this if your cancer is small and your lymph nodes are not able to be felt during clinical examination.
To find the sentinel lymph node, the surgeon usually injects a radioactive tracer and sometimes a dye behind or around the nipple. The injection, which can cause some discomfort, lasts about 15 seconds. The dye or tracer travels to the lymph nodes, arriving at the sentinel node first. If a radioactive tracer is used, it will give off radiation which helps the surgeon find the lymph node. If dye is used, the surgeon can find the lymph node when it turns a blue color.
The pathologist then examines the lymph nodes for cancer cells. If the sentinel lymph node(s) are cancer-free, research has shown that it is likely that the remaining lymph nodes will also be free of cancer. This means that no more lymph nodes need to be removed. If cancer is found in the sentinel lymph node, whether additional surgery is needed to remove more lymph nodes depends on the specific situation. For example, if only 1 or 2 sentinel lymph nodes have cancer and you plan to have a lumpectomy and radiation therapy to the entire breast, an axillary lymph node dissection may not be needed.In general, for many people with early-stage breast cancer with tumors that can be removed with surgery and whose underarm lymph nodes are not enlarged, sentinel lymph node biopsy is the standard of care. However, in certain situations, it may be appropriate to not undergo any axillary surgery. You should talk with your surgeon about whether this may be the right approach for you.
- Axillary lymph node dissection. In an axillary lymph node dissection, the surgeon removes many lymph nodes from under the arm. These are then examined for cancer cells by a pathologist. The actual number of lymph nodes removed varies from person to person. People having a lumpectomy and radiation therapy who have a smaller tumor and 2 or fewer sentinel lymph nodes with cancer may avoid a full axillary lymph node dissection. This helps reduce the risk of side effects and does not decrease survival.
Usually, the lymph nodes are not evaluated for people with DCIS and no invasive cancer, since the risk of spread is very low. However, for patients diagnosed with DCIS who choose to have or need a mastectomy, the surgeon may consider a sentinel lymph node biopsy. If some invasive cancer is found with DCIS during the mastectomy, which happens occasionally, the lymph nodes may then need to be evaluated. However, a sentinel lymph node biopsy generally cannot be performed if the breast has already been removed with mastectomy. In that situation, an axillary lymph node dissection may be recommended.
Most people with invasive breast cancer will have either a sentinel lymph node biopsy or an axillary lymph node dissection. For most people younger than 70 with early-stage breast cancer, a sentinel lymph node biopsy will be used to determine if there is cancer in the axillary lymph nodes, since this information is used to make decisions about treatment. Many patients 70 and older with small hormone receptor-positive and HER2-negative tumors in the breast and no clinically apparent cancer in the lymph nodes can avoid a lymph node evaluation, as the results may not change recommendations for therapies using medication or radiation therapy. Patients age 70 and older with larger hormone receptor-positive and HER2-negative tumors, with other types of breast cancer, or with clinically apparent lymph nodes will generally be recommended to have evaluation of their axillary lymph nodes. Patients should talk with their doctor about recommendations for their specific situation.
No chemotherapy before surgery, and no cancer in the sentinel lymph nodes. For most people in this situation, ASCO does not recommend an axillary lymph node dissection. A small group of patients with tumors located in specific places or with high-risk features may be offered radiation therapy to the lymph nodes.
No chemotherapy before surgery, but there is cancer in the sentinel lymph nodes. If there is cancer in 1 to 2 sentinel lymph nodes, then additional nodal surgery can generally be avoided if the patient is planning to undergo a lumpectomy and receive radiation. If there is cancer in 3 or more sentinel lymph nodes, then ASCO recommends additional nodal surgery.
Chemotherapy is given before surgery. Treatment for people who have received chemotherapy before surgery depends on whether the chemotherapy has destroyed the cancer in the lymph nodes. Therefore, after chemotherapy, patients are often re-staged by sentinel lymph node biopsy. However, this is not always the case. If imaging scans or physical exams suggest abnormal lymph nodes are present, the patient should have an axillary lymph node dissection instead.
-
If there was no evidence of cancer in the lymph nodes either before or after chemotherapy, radiation therapy to the lymph node area is not recommended.
-
If there was evidence of cancer in the lymph nodes before chemotherapy and there is no longer evidence of cancer in the lymph nodes after chemotherapy, radiation therapy to the lymph node area is recommended.
-
If there is evidence of cancer in the lymph nodes after chemotherapy, then both an axillary lymph node dissection and radiation therapy to the lymph node area are recommended.
This information is based on the Ontario Health (Cancer Care Ontario) and ASCO guideline, “ Management of the Axilla in Early-Stage Breast Cancer .” Please note that this link takes you to another ASCO website.
Reconstructive (plastic) surgery
Patients who have a mastectomy or lumpectomy may want to consider breast reconstruction . This is surgery to recreate a breast using either tissue taken from another part of the body or synthetic implants. Reconstruction is usually performed by a plastic surgeon. A reconstruction done at the same time as the mastectomy is called immediate reconstruction. You may also have this surgery done at some point in the future, called delayed reconstruction.
For some patients undergoing a lumpectomy, reconstruction to keep both breasts looking similar is called oncoplastic surgery. This type of surgery may be performed by the breast surgeon.
The techniques discussed below are typically used to shape a new breast.
Implants. A breast implant uses saline-filled or silicone gel-filled forms to reshape the breast. The outside of a saline-filled implant is made up of silicone, and it is filled with sterile saline, which is salt water. Silicone gel-filled implants are filled with silicone instead of saline. There were prior concerns raised that silicone implants might be associated with connective tissue disorders, but clear evidence of this has not been found. Before having permanent implants, a patient may temporarily have a tissue expander placed that will create the correct-sized pocket for the implant. Implants can be placed above or below the pectoralis muscle. Talk with your doctor about the benefits and risks of silicone versus saline implants, and the placement of the implant. The lifespan of an implant depends on the individual. However, some people never need to have them replaced. Other important factors to consider when choosing implants include:
-
Saline implants sometimes "ripple" at the top or shift with time, but many people do not find it bothersome enough to replace.
-
Saline implants feel different than silicone implants. They are often firmer to the touch than silicone implants. If overfilled, they can be firmer, but they can also feel squishier if underfilled.
There can be problems with breast implants. Some people have problems with the shape or appearance. The implants can rupture or break, cause pain and scar tissue around the implant, or get infected. Implants have also been rarely linked to other types of cancer, including a type called breast implant-associated anaplastic large cell lymphoma (BIA-ALCL). Since the risk of developing BIA-ALCL is low, the U.S. Food and Drug Administration (FDA) does not recommend removing textured breast implants or tissue expanders unless there are symptoms. Although these problems are very unusual, talk with your doctor about the risks.
Tissue flap procedures. These techniques use muscle and tissue from elsewhere in the body to reshape the breast. Tissue flap surgery may be done with a “pedicle flap,” which means tissue from the back or belly is moved to the chest without cutting the blood vessels. A “free flap” means the blood vessels are cut and the surgeon needs to attach the moved tissue to new blood vessels in the chest. There are several flap procedures:
-
Transverse rectus abdominis muscle (TRAM) flap. This method, which can be done as a pedicle flap or free flap, uses muscle and tissue from the lower stomach wall.
-
Latissimus dorsi flap . This pedicle flap method uses muscle and tissue from the upper back. Implants are often inserted during this flap procedure.
-
Deep inferior epigastric artery perforator (DIEP) flap . The DIEP free flap takes tissue from the abdomen, and the surgeon attaches the blood vessels to the chest wall.
-
Gluteal free flap. The gluteal free flap uses tissue and muscle from the buttocks to create the breast, and the surgeon also attaches the blood vessels. Transverse upper gracilis (TUG), which uses tissue from the upper thigh, may also be an alternative.
Because blood vessels are involved with flap procedures, these strategies are usually not recommended for people with a
history of diabetes
or connective tissue or vascular disease, or for people who smoke, as the risk of problems during and after surgery is much higher.
The DIEP and other flap procedures take longer to perform in the operating room and have a longer recovery time following surgery. However, the appearance of the breast may be preferred, especially when radiation therapy is part of the treatment plan.
Talk with your doctor for more information about reconstruction options and a referral to a plastic surgeon. When considering a plastic surgeon, choose a doctor who has experience with a variety of reconstructive surgeries, including implants and flap procedures. They can discuss the pros and cons of each procedure.
External breast forms (prostheses)
An external breast prosthesis or artificial breast form provides an option for people who plan to delay or not have reconstructive surgery . These can be made of silicone or soft material, and they fit into a mastectomy bra. Breast prostheses can be made to provide a good fit and natural appearance. Read more about choosing a breast prosthesis.
Flat closure
Some people choose to have a flat closure, also called "going flat," after having a mastectomy instead of having breast reconstruction. This means the surgeon tightens and smooths out the remaining skin, fat, and tissue as much as possible so that the chest wall appears flat. However, a scar will remain.
If you choose to have a flat closure after mastectomy, it is important to go to a surgeon experienced in performing the procedure. Talk with your surgeon about your desired results and ask to see pictures of their work. If you’re not comfortable with the response you receive, consider getting a second opinion.
Deciding to go flat or have breast reconstruction is a personal choice. Each person needs to do what is best for them and choose what honors and respects their values and lifestyle. Learn more about going flat.
Summary of surgical options
To summarize, surgical treatment options include the following:
-
Removal of cancer in the breast: Lumpectomy or partial mastectomy, generally followed by radiation therapy if the cancer is invasive. Mastectomy may also be recommended, with or without immediate reconstruction.
-
Lymph node evaluation: Sentinel lymph node biopsy and/or axillary lymph node dissection.
You are encouraged to talk with your doctor about which surgical option is right for you. Also, talk with your health care team about the possible side effects from the specific surgery you will have and what should be reported to them.
More extensive surgery, such as a mastectomy, is not always better and may cause more complications. The combination of lumpectomy and radiation therapy has a slightly higher risk of the cancer coming back in the same breast or the surrounding area. However, the long-term survival of people who choose to have a lumpectomy is exactly the same as those who have a mastectomy. Even with a mastectomy, not all breast tissue can be removed, and there is still a chance of recurrence or of developing a new breast cancer.
People with a very high risk of developing a new cancer in the other breast may consider a bilateral mastectomy, meaning both breasts are removed. This includes people with BRCA1 and BRCA2 gene mutations and people with cancer in both breasts. People with BRCA1 or BRCA2 gene mutations should talk with their doctor about which surgical option might be best for them, as they have an increased risk of developing breast cancer in the opposite breast and of developing a new breast cancer in the same breast compared to those without these mutations. ASCO recommends that people with a BRCA1 or BRCA2 gene mutation who are being treated with a mastectomy for the breast with cancer should also be offered a risk-reducing mastectomy for the opposite breast, including nipple-sparing mastectomy. This is because getting a risk-reducing mastectomy in the opposite breast is associated with a decreased risk of getting cancer in that breast. However, not everyone will be a good candidate for nipple-sparing mastectomy, either because of characteristics of their cancer or because of factors related to their breast anatomy. For example, people with large breasts and little nipple projection may need a breast reduction prior to undergoing nipple-sparing mastectomy.
To assess your risk of developing cancer in the opposite breast and determine whether you might be eligible for a risk-reducing mastectomy, your doctor will consider several factors:
-
Age of diagnosis
-
Family history of breast cancer
-
The likelihood of recurrence of your breast cancer or other cancers you may have, such as ovarian cancer
-
Your ability to have regular surveillance studies, such as breast MRI, to look for breast cancer
-
Any other diseases or conditions you might have
-
Life expectancy
People with a moderate-risk gene mutation, like PALB2 , CHEK2 or ATM , should also talk with their doctor and genetic counselor about their risk of developing breast cancer in the opposite breast and whether undergoing a risk-reducing mastectomy, including a nipple-sparing mastectomy, may be right for them.
People with a high-risk mutation who do not have a bilateral mastectomy should have regular screening of the remaining breast tissue with an annual mammogram and breast MRI for enhanced surveillance.
For people who are not at very high risk of developing a new cancer in the future, having a healthy breast removed in a bilateral mastectomy neither prevents cancer recurrence nor improves their survival. It also will not change the recommendation for treatment of the cancer with medications such as chemotherapy and hormonal therapy. Although the risk of getting a new cancer in that breast will be lowered, surgery to remove the other breast does not reduce the risk of the original cancer coming back. Survival is based on the prognosis of the initial cancer. In addition, more extensive surgery may be linked with a greater risk of problems. Read more about talking with your doctor about breast surgery options.
This information is based on ASCO’s recommendations for the management of hereditary breast cancer. Please note that this link takes you to a separate ASCO website.
Return to top
Radiation therapy
Radiation therapy is the use of high-energy x-rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. There are several different types of radiation therapy:
-
Whole breast irradiation. Whole breast irradiation is external-beam radiation therapy that is given to the entire breast. External-beam radiation therapy is the most common type of radiation treatment and is given from a machine outside the body. As described below, whole breast irradiation can be given using a number of different treatment schedules.
-
Partial breast irradiation. Partial breast irradiation (PBI) is radiation therapy that is given directly to the tumor area instead of the entire breast. It is more common after a lumpectomy. Targeting radiation directly to the tumor area usually shortens the amount of time that patients need to receive radiation therapy. However, only some patients may be able to have PBI. Although early results have been promising, PBI is still being studied. PBI can be given using external-beam or intra-operative radiation therapy or brachytherapy.
-
Intra-operative radiation therapy. This is when radiation treatment is given using a probe in the operating room.
-
Brachytherapy. This type of radiation therapy is given by placing radioactive sources into the tumor.
Although the research results are encouraging, intra-operative radiation therapy and brachytherapy are not widely used. Where available, they may be options for a patient with a small tumor that has not spread to the lymph nodes. You may want to discuss with your radiation oncologist the pros and cons of PBI compared to whole breast radiation therapy.
-
-
Intensity-modulated radiation therapy. Intensity-modulated radiation therapy (IMRT) is a more advanced way to give external-beam radiation therapy to the breast. The intensity of the radiation directed at the breast is varied to better target the tumor, spreading the radiation more evenly throughout the breast. The use of IMRT lessens the radiation dose and may decrease possible damage to nearby organs, such as the heart and lung, as well as lessen the risks of some immediate side effects, such as peeling of the skin during treatment. This can be especially important for people with medium to large breasts who have a higher risk of side effects, such as peeling and burns, compared with people with smaller breasts. IMRT may also help to lessen the long-term effects on the breast tissue, such as hardness, swelling, or discoloration, that were common with older radiation techniques.
IMRT is not recommended for everyone. Talk with your radiation oncologist to learn more. Special insurance approval may also be needed for coverage for IMRT. It is important to check with your health insurance company before any treatment begins to make sure it is covered.
-
Proton therapy. Standard radiation therapy for breast cancer uses x-rays, also called photon therapy, to kill cancer cells. Proton therapy is a type of external-beam radiation therapy that uses protons rather than x-rays. At high energy, protons can destroy cancer cells. Protons have different physical properties that may allow the radiation therapy to be more targeted than photon therapy and potentially reduce the radiation dose. The therapy may also reduce the amount of radiation that goes near the heart. Researchers are studying the benefits of proton therapy versus photon therapy in a national clinical trial. Currently, proton therapy is an experimental treatment and may not be widely available or covered by health insurance.
Learn more about the basics of radiation therapy .
A radiation therapy regimen, or schedule (see below), usually consists of a specific number of treatments given over a set period of time. Treatment is most often given once a day, 5 days a week, for 1 to 6 weeks. Radiation therapy often helps lower the risk of recurrence in the breast. In fact, with modern surgery and radiation therapy, recurrence rates in the breast are now less than 5% in the 10 years after treatment or 6% to 7% at 20 years. Survival is the same with lumpectomy or mastectomy. If there is cancer in the lymph nodes under the arm, radiation therapy may also be given to the same side of the neck or underarm near the breast or chest wall.
Radiation therapy may be given after or before surgery:
-
Adjuvant radiation therapy is given after surgery. Most patients who have a lumpectomy also have radiation therapy. Patients who have a mastectomy may or may not need radiation therapy, depending on the features of the tumor. Radiation therapy may be recommended after mastectomy if a patient has a larger tumor, cancer in the lymph nodes, cancer cells outside of the capsule of the lymph node, or cancer that has grown into the skin or chest wall, as well as for other reasons. When patients are also recommended to have adjuvant chemotherapy, radiation therapy is usually given after chemotherapy is complete. Radiation therapy after surgery for DCIS may or may not be offered depending on the risk of recurrence.
-
Neoadjuvant radiation therapy is radiation therapy given before surgery to shrink a large tumor, which makes it easier to remove. This approach is uncommon and is usually only considered when a tumor cannot be removed with surgery.
Radiation therapy can cause side effects, including fatigue, swelling of the breast, redness and/or skin discoloration, and pain or burning in the skin where the radiation was directed, sometimes with blistering or peeling. Your doctor can recommend topical medication to apply to the skin to treat some of these side effects. Following radiation therapy, the breast can feel firmer or the skin of the breast can feel thicker.
Very rarely, a small amount of the lung can be affected by the radiation therapy, causing pneumonitis, a radiation-related swelling of the lung tissue. This risk depends on the size of the area that received radiation therapy, and it tends to heal with time.
In the past, with older equipment and radiation therapy techniques, people who received treatment for breast cancer on the left side of the body had a small increase in the long-term risk of heart disease. Modern techniques, such as respiratory gating, which uses technology to guide the delivery of radiation while a patient breathes, are now able to spare the vast majority of the heart from the effects of radiation therapy.
Many types of radiation therapy may be available to you with different schedules (see below). Talk with your doctor about the advantages and disadvantages of each option.
Radiation therapy schedule
Radiation therapy is usually given daily for a set number of weeks.
-
After a lumpectomy. Radiation therapy after a lumpectomy is external-beam radiation therapy generally given Monday through Friday for 3 to 4 weeks if the cancer is not in the lymph nodes. If the cancer is in the lymph nodes, radiation therapy is often given for 5 to 6 weeks. However, these durations are changing, as there is a preference for a shorter duration to be given in patients who meet the criteria for shorter treatment. This often starts with radiation therapy to the whole breast, followed by a more focused treatment to where the tumor was located in the breast for the remaining treatments.
This focused part of the treatment, called a boost, is standard for most patients with invasive breast cancer to reduce the risk of a recurrence in the breast. People with DCIS may also receive the boost. For patients with a low risk of recurrence, the boost may be optional. It is important to discuss this treatment approach with your doctor.
-
After a mastectomy. For those who need radiation therapy after a mastectomy, it is usually given 5 days a week for 5 to 6 weeks. Radiation therapy can be given before or after reconstructive surgery. As is the case following lumpectomy, some patients may be recommended to have less than 5 weeks of radiation therapy after mastectomy.
Even shorter schedules have been studied and are in use in some centers, including accelerated partial breast radiation therapy for 5 days.
These shorter schedules may not be options for patients who need radiation therapy after a mastectomy or radiation therapy to their lymph nodes. Also, longer schedules of radiation therapy may be needed for some people.
Adjuvant radiation therapy concerns for older patients and/or those with a small tumor
Recent research studies have looked at the possibility of avoiding radiation therapy for people age 65 or older with an ER-positive, lymph node-negative, early-stage tumor (see Introduction ), or for people with a small tumor. Importantly, these studies show that for people with small, less aggressive breast tumors that are removed with lumpectomy, the likelihood of cancer returning in the same breast is very low. Treatment with radiation therapy reduces the risk of breast cancer recurrence in the same breast even further compared with surgery alone. However, radiation therapy does not lengthen a person's life.
Guidelines from the National Comprehensive Cancer Network (NCCN) continue to recommend radiation therapy as the standard option after lumpectomy. However, they note that people with special situations or a low-risk tumor could reasonably choose not to have radiation therapy and use only systemic medication therapy (see below) after lumpectomy. This includes people age 70 or older, as well as those with medical conditions that could limit life expectancy within 5 years. People who choose this option will have a modest increase in the risk of the cancer coming back in the breast. It is important to discuss the pros and cons of omitting radiation therapy with your doctor.
Adjuvant radiation therapy for those with a genetic mutation
ASCO recommends that, when appropriate, adjuvant radiation therapy should be offered to people with breast cancer with a BRCA1 or BRCA2 mutation. People with a TP53 mutation are at higher risk of complications from radiation therapy, and therefore should undergo mastectomy instead of lumpectomy and radiation. Those with an ATM mutation or other related mutations should talk with their doctor about whether adjuvant radiation therapy is right for them. Currently, there is not enough data to recommend avoiding radiation therapy in all people with ATM mutations.
Return to top
Therapies using medication
The treatment plan may include medications to destroy cancer cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy. Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body. However, this is almost never done in breast cancer treatment.
This treatment is generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication. Medications are often given through an intravenous (IV) tube placed into a vein using a needle, an injection into a muscle or under the skin, or as a pill or capsule that is swallowed (orally). If you are given oral medications, be sure to ask your health care team about how to safely store and handle them.
The types of medications used for breast cancer include:
-
Chemotherapy
-
Hormonal therapy
-
Targeted therapy
-
Immunotherapy
Each of these therapies for treatment of non-metastatic breast cancer is discussed below in more detail. A person may receive 1 type of medication at a time or a combination of medications given at the same time. They can also be given as part of a treatment plan that includes surgery and/or radiation therapy. Different drugs or combinations of drugs are use to treat metastatic disease. Information about these therapies can be found in this website's Guide to Metastatic Breast Cancer .
The medications used to treat cancer are continually being evaluated. Your doctor may suggest that you consider participating in clinical trials that are studying new ways to treat breast cancer. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purposes, and their potential side effects or interactions with other medications.
It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases .
Chemotherapy
Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells. It may be given before surgery to shrink a large tumor, make surgery easier, and/or reduce the risk of recurrence. When it is given before surgery, it is called neoadjuvant chemotherapy. It may also be given after surgery to reduce the risk of recurrence, called adjuvant chemotherapy.
A neoadjuvant or adjuvant chemotherapy regimen, or schedule, usually consists of a combination of drugs given in a specific number of cycles over a set period of time. Chemotherapy may be given on many different schedules depending on what worked best in clinical trials for that specific type of regimen. It may be given once a week, once every 2 weeks, or once every 3 weeks. There are many types of chemotherapy used to treat breast cancer. Common drugs include the following, most of which are available as a generic drug:
-
Doc etaxel
-
Paclitaxel
-
Doxorubicin
-
Epirubicin
-
Capecitabine
-
Carboplatin
-
Cyclophosphamide
-
Fluorouracil (5-FU)
-
Methotrexate
-
Protein-bound paclitaxel
A patient may receive 1 drug or a combination of different drugs given at the same time to treat their cancer. Research has shown that combinations of certain drugs are sometimes more effective than single drugs for adjuvant treatment.
The following drugs or combinations of drugs may be used as neoadjuvant or adjuvant therapy for early-stage and locally advanced breast cancer:
-
AC (doxorubicin and cyclophosphamide)
-
EC (epirubicin, cyclophosphamide)
-
AC or EC followed by T (paclitaxel or docetaxel), or the reverse
-
AC or EC followed by T (paclitaxel or docetaxel) and carboplatin, or the reverse
-
CAF (cyclophosphamide, doxorubicin, and 5-FU)
-
CEF (cyclophosphamide, epirubicin, and 5-FU)
-
CMF (cyclophosphamide, methotrexate, and 5-FU)
-
TAC (docetaxel, doxorubicin, and cyclophosphamide)
-
TC (docetaxel and cyclophosphamide)
-
Capecitabine (Xeloda)
Therapies that target the HER2 receptor may be given with chemotherapy for HER2-positive breast cancer (see "Targeted therapy," below). An example is the antibody trastuzumab. Combination regimens for early-stage HER2-positive breast cancer may include:
-
AC-TH (doxorubicin, cyclophosphamide, paclitaxel or docetaxel, trastuzumab)
-
AC-THP (doxorubicin, cyclophosphamide, paclitaxel or docetaxel, trastuzumab, pertuzumab)
-
TCH (paclitaxel or docetaxel, carboplatin, trastuzumab)
-
TCHP (paclitaxel or docetaxel, carboplatin, trastuzumab, pertuzumab)
-
TH (paclitaxel, trastuzumab)
Immunotherapies may be given with chemotherapy for triple negative breast cancer (see "Immunotherapy," below). An example is the antibody pembrolizumab. Combination regimens for triple negative breast cancer may include:
-
TC/pembro-AC/pembro (paclitaxel and carboplatin plus pembrolizumab followed by doxorubicin and cyclophosphamide plus pembrolizumab)
-
TC/pembro-EC/pembro (paclitaxel and carboplatin plus pembrolizumab followed by epirubicin and cyclophosphamide plus pembrolizumab)
The side effects of chemotherapy depend on the individual, the drug(s) used, whether the chemotherapy has been combined with other drugs, and the schedule and dose used. These side effects can include fatigue, risk of serious infection, nausea and vomiting, hair loss, loss of appetite, diarrhea, constipation, numbness and tingling, pain, early menopause, weight gain, and chemo-brain or cognitive dysfunction. These side effects can often be very successfully prevented or managed during treatment with supportive medications, and they usually go away after treatment is finished. For some people, numbness and tingling can remain after chemotherapy. For hair loss reduction, talk with your doctor about whether the center does cold cap or scalp cooling techniques. Rarely, long-term side effects may occur, such as heart damage or secondary cancers such as leukemia or lymphoma.
Many patients feel well during chemotherapy and are active, including taking care of their families, working, and exercising during treatment, although each person’s experience can be different. Talk with your health care team about the possible side effects of your specific chemotherapy plan, and seek medical attention immediately if you experience a fever during chemotherapy.
Learn more about the basics of chemotherapy .
Return to top
Hormonal therapy
Hormonal therapy, also called endocrine therapy, is an effective treatment for most tumors that test positive for either estrogen or progesterone receptors (called ER positive or PR positive; see Introduction ). This type of tumor uses hormones to fuel its growth. Blocking the hormones can help prevent a cancer recurrence and death from breast cancer when hormonal therapy is used either by itself or after chemotherapy.
Hormonal therapy for breast cancer treatment is different than menopausal hormone therapy (MHT). MHT may also be called postmenopausal hormone therapy or hormone replacement therapy (HRT). Hormonal therapies used in breast cancer treatment act as “anti-hormone” or “anti-estrogen” therapies. They block hormone actions or lower hormone levels in the body. Hormonal therapy may also be called endocrine therapy. The endocrine system in the body makes hormones. Learn more about the basics of hormone therapy .
Hormonal therapy may be given before surgery to shrink a tumor, make surgery easier, and/or lower the risk of recurrence. This is called neoadjuvant hormonal therapy. When given before surgery, it is typically given for at least 3 to 6 months before surgery and continued after surgery. It may also be given solely after surgery to reduce the risk of recurrence. This is called adjuvant hormonal therapy.
Types of hormonal therapy
-
Tamoxifen. Tamoxifen is a drug that blocks estrogen from binding to breast cancer cells. It is effective for lowering the risk of recurrence in the breast that had cancer, the risk of developing cancer in the other breast, and the risk of distant recurrence. Tamoxifen works in people who have been through menopause as well as those who have not.
Tamoxifen is a pill that is taken daily by mouth every day for 5 to 10 years. For premenopausal people, it may be combined with medication to stop the ovaries from producing estrogen. It is important to discuss any other medications or supplements you take with your doctor, as there are some that may interfere with tamoxifen. Common side effects of tamoxifen include hot flashes and vaginal dryness, discharge, or bleeding. Very rare risks include a cancer of the lining of the uterus, cataracts, and blood clots. However, tamoxifen may improve bone health and cholesterol levels in postmenopausal people.
-
Aromatase inhibitors (AIs). AIs decrease the amount of estrogen made in tissues other than the ovaries in post-menopausal people by blocking the aromatase enzyme. This enzyme changes weak male hormones called androgens into estrogen. These drugs include anastrozole (Arimidex), exemestane (Aromasin), and letrozole (Femara). All of the AIs are pills taken daily by mouth. Only patients who have gone through menopause or who take medicines to stop the ovaries from making estrogen (see "Ovarian suppression," below) can take AIs. Treatment with AIs, either as the first hormonal therapy taken or after treatment with tamoxifen, may be more effective than taking only tamoxifen to reduce the risk of recurrence in post-menopausal people.
The side effects of AIs may include muscle and joint pain, hot flashes, vaginal dryness, an increased risk of osteoporosis and broken bones, and rarely, increased cholesterol levels and thinning of hair. Research shows that all AIs work equally well and have similar side effects. However, people who have undesirable side effects while taking one AI medication may have fewer side effects with a different AI for unclear reasons.
Patients who have not gone through menopause and who are not getting shots to stop the ovaries from working (see below) should not take AIs, as they do not block the effects of estrogen made by the ovaries. Often, doctors will monitor blood estrogen levels in people whose menstrual cycles have recently stopped, those whose periods stopped with chemotherapy, or those who have had a hysterectomy but their ovaries are still in place, to be sure that the ovaries are no longer producing estrogen. -
Ovarian suppression or ablation. Ovarian suppression is the use of drugs to stop the ovaries from producing estrogen. Ovarian ablation is the use of surgery to remove the ovaries. These options may be used in addition to another type of hormonal therapy for people who have not been through menopause.
-
For ovarian suppression, gonadotropin or luteinizing releasing hormone (GnRH or LHRH) agonist drugs are used to stop the ovaries from making estrogen, causing temporary menopause. Goserelin (Zoladex) and leuprolide (Eligard, Lupron) are types of these drugs. They are typically given in combination with other hormonal therapy, not alone. They are given by injection every 4 or 12 weeks and stop the ovaries from making estrogen. The effects of GnRH drugs go away if treatment is stopped.
-
For ovarian ablation, surgery to remove the ovaries is used to stop estrogen production. While this is permanent, it can be a good option for people who no longer want to become pregnant to consider. The cost is typically lower over the long term.
-
Hormonal therapy after menopause
People who have gone through menopause and are prescribed hormonal therapy have several options:
-
Tamoxifen for 5 to 10 years
-
An AI for 5 to 10 years
-
Tamoxifen for 5 years, followed by an AI for up to 5 years. This would be a total of 10 years of hormonal therapy.
-
Tamoxifen for 2 to 3 years, followed by 2 to 8 years of an AI for a total of 5 to 10 years of hormonal therapy.
In general, patients should expect 5 to 10 years of hormonal therapy. The tumor biomarkers and other features of the cancer may also impact who is recommended to take a longer course of hormonal therapy.
Hormonal therapy before menopause
As noted above, premenopausal patients should not take AI medications without ovarian suppression, as they will not lower estrogen levels. Options for adjuvant hormonal therapy for premenopausal people include the following:
-
Tamoxifen for 5 years. Then, treatment is based on their risk of cancer recurrence as well as whether or not they have gone through menopause during those first 5 years.
-
If a person has not gone through menopause after the first 5 years of treatment and is recommended to continue treatment, they can continue tamoxifen for another 5 years, for a total of 10 years of tamoxifen. Alternatively, a person could start ovarian suppression and switch to taking an AI for another 5 years.
-
If a person goes through menopause during the first 5 years of treatment and is recommended to continue treatment, they can continue tamoxifen for an additional 5 years or switch to an AI for 5 more years. This would be a total of 10 years of hormonal therapy. Only people who are clearly post-menopausal should consider taking an AI.
-
Some patients are recommended to stop all hormonal therapy treatment after the first 5 years of tamoxifen.
-
-
Ovarian suppression for 5 years along with additional hormonal therapy, such as tamoxifen or an AI, may be recommended in the following situations, depending on a person’s age and risk of recurrence:
-
For people who are diagnosed with breast cancer at a very young age.
-
For people who have a high risk of cancer recurrence.
-
For people with stage II or stage III cancer when chemotherapy is also recommended. However, evidence now suggests benefits independent of the use of chemotherapy as well.
-
For people with stage I or stage II cancer with a higher risk of recurrence who may consider also having chemotherapy.
-
For people who cannot take tamoxifen for other health reasons, such as having a history of blood clots. They would take an AI medication in addition to ovarian suppression.
-
-
Ovarian suppression is not recommended in addition to another type of hormonal therapy in the following situations:
-
For people with cancer that is not very likely to recur.
-
For people with stage I cancer when chemotherapy has not been recommended.
-
Additional targeted therapy in combination with hormone therapy
The following drug is used in combination with hormonal therapy for the treatment of non-metastatic hormone receptor-positive and HER2-negative breast cancer and a high risk of breast cancer recurrence.
-
Abemaciclib (Verzenio). This oral drug, called a CDK4/6 inhibitor, targets a protein in breast cancer cells called CDK4/6, which may stimulate cancer cell growth. It is approved as treatment in combination with hormonal therapy (tamoxifen or an AI) to treat people with hormone receptor-positive, HER2-negative, early breast cancer that has spread to the lymph nodes and has a high risk of recurrence. It can cause diarrhea, low blood count, fatigue, and other symptoms. ASCO recommends consideration of 2 years of treatment with abemaciclib combined with 5 or more years of hormonal therapy for patients meeting these criteria, including for people whose cancer has a Ki-67 score higher than 20% (see Diagnosis ).
This information is based on ASCO recommendations for adjuvant endocrine therapy for women with hormone receptor-positive breast cancer . Please note this link takes you to another ASCO website.
Hormonal therapy for treatment of metastatic hormone receptor-positive breast cancer is described in the Guide to Metastatic Breast Cancer .
Learn more about the basics of hormonal therapy .
Return to top
Targeted therapy
Targeted therapy is a treatment that targets the cancer’s specific genes, proteins, or the tissue environment that contributes to cancer growth and survival. These treatments are very focused and work differently than chemotherapy. This type of treatment blocks the growth and spread of cancer cells and limits damage to healthy cells.
Not all tumors have the same targets. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. In addition, research studies continue to find out more about specific molecular targets and new treatments directed at them. Learn more about the basics of targeted treatments .
The first approved targeted therapies for breast cancer were hormonal therapies. Then, HER2-targeted therapies were approved to treat HER2-positive breast cancer.
HER2-targeted therapy
-
Trastuzumab (FDA-approved biosimilar forms are available). This drug is approved as a therapy for non-metastatic, HER2-positive breast cancer. It is given either as an infusion into a vein every 1 to 3 weeks or as an injection into the skin every 3 weeks. Currently, patients with stage I to stage III breast cancer (see Stages ) should receive a trastuzumab-based regimen, often including a combination of trastuzumab with chemotherapy, followed by a total of 1 year of adjuvant HER2-targeted therapy. Patients receiving trastuzumab have a small (2% to 5%) risk of heart problems. This risk is increased if a patient has other risk factors for heart disease or receives chemotherapy that also increases the risk of heart problems at the same time. These heart problems may go away and can be treated with medication.
-
Pertuzumab (Perjeta). This drug is approved for stage II and III breast cancer in combination with trastuzumab and chemotherapy. It is given as an infusion into a vein every 3 weeks.
-
Pertuzumab, trastuzumab, and hyaluronidase–zzxf (Phesgo). This combination drug, which contains pertuzumab, trastuzumab, and hyaluronidase-zzxf in a single dose, is approved for people with early-stage HER2-positive breast cancer. It may be given in combination with chemotherapy. It is given by injection under the skin and can be administered either at a treatment center or at home by a health care professional.
-
Neratinib (Nerlynx). This oral drug is approved as a treatment for higher-risk HER2-positive, early-stage breast cancer. It is taken for a year, starting after patients have finished 1 year of trastuzumab.
-
Ado-trastuzumab emtansine or T-DM1 (Kadcyla). This is approved for patients with early-stage breast cancer who have had treatment with trastuzumab and chemotherapy with either paclitaxel or docetaxel followed by surgery, and who had cancer remaining (or present) at the time of surgery. ASCO recommends that these patients receive 14 cycles of T-DM1 after surgery unless the cancer recurs or the side effects from T-DM1 become too difficult to manage. T-DM1 is a combination of trastuzumab linked to a very small amount of a strong chemotherapy. This allows the drug to deliver chemotherapy into the cancer cell while lessening the chemotherapy received by healthy cells, which usually means that it causes fewer side effects than standard chemotherapy. T-DM1 is given by vein every 3 weeks.
This information is based on the ASCO guideline, “ Selection of Optimal Adjuvant Chemotherapy and Targeted Therapy for Early Breast Cancer .” Please note that this link takes you to another ASCO website.
Talk with your doctor about possible side effects of specific medications and how they can be managed.
Bone modifying drugs
Bone modifying drugs block bone destruction and help strengthen the bone. These medications, called bisphosphonates, may also be used to prevent cancer from recurring in the bone. Bone modifying drugs are not a substitute for standard anti-cancer treatments. Certain types of bone modifying drugs are also used in low doses to prevent and treat osteoporosis, which is the thinning of the bones.
All people with breast cancer who have been through menopause, regardless of the cancer’s hormone receptor status and HER2 status, should have a discussion with their doctor whether bisphosphonates are right for them. Several factors affect this decision, including your risk of recurrence, the side effects of treatment, the cost of treatment, your preferences, and your overall health.
If treatment with bisphosphonates is recommended, ASCO recommends starting within 3 months after surgery or within 2 months after adjuvant chemotherapy. This may include treatment with clodronate (multiple brand names), ibandronate (Boniva), or zoledronic acid (Zometa). Clodronate is not available in the United States.
This information is based on the ASCO and Ontario Health (Cancer Care Ontario) guideline, “ Use of Adjuvant Bisphosphonates and Other Bone-Modifying Agents in Breast Cancer .” Please note that this link takes you to another ASCO website.
Other types of targeted therapy for breast cancer
You may have other targeted therapy options for breast cancer treatment, depending on several factors. The following drug is used for the treatment of non-metastatic breast cancer in people with an inherited BRCA1 or BRCA2 gene mutation and a high risk of breast cancer recurrence.
-
Olaparib (Lynparza). This is a type of oral drug called a PARP inhibitor, which destroys cancer cells by preventing them from fixing damage to the cells. ASCO recommends using olaparib to treat early-stage, HER2-negative breast cancer in people with an inherited BRCA1 or BRCA2 gene mutation and a high risk of breast cancer recurrence. Adjuvant olaparib should be given for 1 year following the completion of chemotherapy, surgery, and radiation therapy (if needed).
You can learn more about drugs used to treat metastatic breast cancer in the Guide to Metastatic Breast Cancer .
Return to top
Immunotherapy
Immunotherapy uses the body's natural defenses to fight cancer by improving your immune system’s ability to attack cancer cells. The following drug, which is a type of immunotherapy called an immune checkpoint inhibitor, is used for the treatment of high-risk, early-stage, triple-negative breast cancer.
-
Pembrolizumab (Keytruda). This is a type of immunotherapy that is approved by the FDA to treat high-risk, early-stage, triple-negative breast cancer in combination with chemotherapy before surgery. It is then continued following surgery for 9 doses.
Common side effects include skin rashes, flu-like symptoms, thyroid problems, diarrhea, and weight changes. Other severe but less common side effects can also occur. Talk with your doctor about possible side effects of the immunotherapy recommended for you and what can be done to watch for and manage them. Learn more about the basics of immunotherapy .
Return to top
Neoadjuvant systemic therapy for non-metastatic breast cancer
Neoadjuvant systemic therapy is treatment given before surgery to shrink a large tumor and/or reduce the risk of recurrence. Chemotherapy, immunotherapy, hormonal therapy, and/or targeted therapy may all be given as neoadjuvant treatments for people with certain types of breast cancer.
Neoadjuvant chemotherapy, for example, is the treatment usually recommended for people with inflammatory breast cancer . It is also the treatment recommended for people with locally advanced cancer (large tumor(s) and/or several lymph nodes affected) or cancer that would be difficult to remove with surgery at the time of diagnosis but may become removable with surgery after receiving neoadjuvant treatment. The doctor will consider several factors, including the type of breast cancer that you have, such as its grade, stage, and estrogen, progesterone, and HER2 status, to guide their recommendation around whether neoadjuvant chemotherapy should be part of your treatment plan.
ASCO recommends that neoadjuvant systemic therapy be offered to people with high-risk HER2-positive breast cancer or to people with triple-negative breast cancer who would then receive additional drug therapy after surgery if cancer still remains. Neoadjuvant therapy may also be offered to reduce the amount of surgery that needs to be performed and allow someone who would otherwise require a mastectomy, for example, to consider having a lumpectomy.
In situations where delaying surgery is preferred (such as waiting for genetic test results to guide further treatment options or to allow time for deciding on breast reconstruction options), neoadjuvant systemic therapy may be offered.
People receiving neoadjuvant chemotherapy should be monitored for the cancer’s response to treatment through regular examinations. Your doctor will likely suggest breast imaging after treatment for surgical planning. They may also perform imaging if they are concerned that the cancer may have progressed despite treatment. Your doctor will likely use the same type of imaging test in your follow-up care that was most helpful at the time your breast cancer was originally diagnosed. In general, it is not recommended that blood tests or biopsies be used to monitor response to therapy for people receiving neoadjuvant chemotherapy.
Neoadjuvant systemic therapy options by type of non-metastatic breast cancer
For triple-negative breast cancer:
For patients with triple-negative breast cancer that has spread to the lymph nodes and/or is more than 1 centimeter (cm) in size, ASCO recommends they be offered neoadjuvant chemotherapy. Additional drugs, including the chemotherapy drug carboplatin and the immunotherapy drug pembrolizumab (see above), may also be recommended in addition to usual chemotherapy drugs to increase the likelihood of having a complete response and reduce the risk of cancer returning. A complete response is when there is no cancer found in the tissue when it is removed during surgery. Talk with your doctor about the potential benefits and risks of receiving carboplatin and pembrolizumab before surgery.
People with early-stage (1 cm or less, and no lymph nodes that look abnormal) triple-negative breast cancer should not routinely be offered neoadjuvant therapy unless they are participating in a clinical trial.
For HER2-negative, hormone receptor-positive breast cancer:
In cases where a recommendation for chemotherapy can be made without having all the information that is obtained from surgery, such as the actual size of the tumor or the number of involved lymph nodes, any person with HER2-negative, hormone receptor-positive breast cancer can receive neoadjuvant chemotherapy instead of adjuvant chemotherapy. Meanwhile, for postmenopausal people with large tumors or other reasons why surgery may not be a good option at the time of diagnosis of the cancer, hormonal therapy with an aromatase inhibitor may be offered to reduce the size of the tumor. It may also be used to control the cancer if there is no role for surgery. However, hormonal therapy should not be routinely offered in this situation outside of a clinical trial for premenopausal people with early-stage HER2-negative, hormone receptor-positive breast cancer.
For HER2-positive breast cancer:
For patients with HER2-positive breast cancer that has spread to the lymph nodes or is more than 2 cm in size, neoadjuvant therapy with chemotherapy in combination with the targeted therapy drug trastuzumab should be offered. Another targeted therapy drug against HER2, pertuzumab, may also be used with trastuzumab when given before surgery. However, people with early stage (1 cm or smaller and no abnormal appearing lymph nodes), HER2-positive cancer should not be routinely offered neoadjuvant chemotherapy or drugs that target HER2 (such as trastuzumab and pertuzumab) outside of a clinical trial.
This information is based on the ASCO guideline, “ Neoadjuvant Chemotherapy, Endocrine Therapy, and Targeted Therapy for Breast Cancer .” Please note that this link takes you to another ASCO website.
Return to top
Systemic therapy concerns for people age 65 or older
Age should never be the only factor used to determine treatment options. Systemic treatments, such as chemotherapy, often work as well for older patients as they do for younger patients. However, older patients may be more likely to have side effects that impact their quality of life. Older patients may also have a higher risk of drug-associated toxicities.
For example, older patients may have a higher risk of developing heart problems from trastuzumab. This is more common for patients who already have heart disease and for those who receive certain combinations of chemotherapy. For older patients receiving chemotherapy, they may have a higher risk of fatigue and peripheral neuropathy. Learn more in this separate article on this website.
It is important for all patients to talk with their doctors about the systemic therapy options being recommended, including the benefits and risks. They should also ask about potential side effects and how they can be managed. Learn more about cancer and aging .
Return to top
Physical, emotional, and social effects of cancer ( updated 08/2023 )
In general, cancer and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Supportive care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after a cancer diagnosis. People who receive supportive care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Supportive care treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies.
Research has shown that some
integrative or complementary therapies
may be helpful to manage symptoms and side effects. Integrative medicine is the combined use of medical treatment for the cancer along with complementary therapies, such as mind-body practices, natural products, and/or lifestyle changes. However, most natural products are unregulated, so the risk of them interacting with your treatment and causing harm is uncertain.
ASCO agrees with recommendations from
the Society for Integrative Oncology (SIO)
on several complementary options to help manage general side effects during and after breast cancer treatment. These include:
-
Music therapy, mindfulness meditation, stress management, and yoga for reducing stress
-
Mindfulness meditation and yoga to improve general quality of life
-
Acupressure and acupuncture to help with nausea and vomiting from chemotherapy
Specifically for managing anxiety and depression, ASCO and SIO recommend several complementary options to help manage these side effects during and after breast cancer treatment. These include the following for helping with anxiety or depression symptoms:
-
For reducing anxiety during breast cancer treatment: mind-body techniques like deep breathing, mindfulness meditation practices, yoga, hypnosis, music therapy, reflexology, and lavender essential oil
-
For reducing anxiety after breast cancer treatment: mindfulness-based stress reduction meditation practices, acupuncture, tai chi, qigong, and reflexology
-
For reducing symptoms of depression during breast cancer treatment: mindfulness-based stress reduction meditation practices, yoga, music therapy, relaxation techniques like deep breathing, and reflexology
-
For reducing symptoms of depression after breast cancer treatment: mindfulness meditation practices, yoga, tai chi, and qigong
There are other techniques or practices that may help reduce anxiety or symptoms of depression during or after cancer. However, there are no specific recommendations for them, so be sure to talk with your health care team about whether any additional techniques may be helpful for you.
Learn more about the recommendations for using integrative therapy for breast cancer from an
SIO guideline
and from a
joint SIO-ASCO guideline
. (Note that these links will take you to different ASCO websites.)
People may have concerns about if or how their treatment may affect their sexual health and their ability to have children in the future , called fertility. People are encouraged to talk with their health care team about these topics prior to starting treatment.
Before treatment begins, talk with your doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and symptom management options. Many people also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about supportive care or palliative care in a separate section of this website.
Return to top
Recurrent breast cancer
If the cancer returns after treatment for early-stage disease, it is called recurrent cancer. When breast cancer recurs, it may come back in the following parts of the body:
-
The same place as the original cancer. This is called a local recurrence.
-
The chest wall or lymph nodes under the arm or in the chest on the same side as the original cancer. This is called a regional recurrence.
-
Another place, including distant organs such as the bones, lungs, liver, and brain. This is called a distant recurrence or a metastatic recurrence. For more information on a metastatic recurrence, see the Guide to Metastatic Breast Cancer .
If a recurrence happens, a new cycle of testing will begin again to learn as much as possible about it. Testing may include imaging tests, such as those discussed in the Diagnosis section. In addition, another biopsy will likely be needed to confirm the breast cancer recurrence and learn about the features of the cancer.
After this testing is done, you and your doctor will talk about the treatment options. The treatment plan may include the treatments described above, such as surgery, radiation therapy, chemotherapy, targeted therapy, and hormonal therapy. They may be used in a different combination or given at a different pace. The treatment options for recurrent breast cancer depend on the following factors:
-
Previous treatment(s) for the cancer first diagnosed
-
Time since the first diagnosis
-
Location of the recurrence
-
Characteristics of the tumor, such as ER, PR, and HER2 status
-
Results from previous genomic tests
-
Depending on the type of breast cancer, your doctor may recommend testing for the following molecular features:
-
PD-L1. PD-L1 is found on the surface of cancer cells and some of the body's immune cells. This protein stops the body’s immune cells from destroying the cancer, especially in triple-negative breast cancer.
-
Microsatellite instability-high (MSI-H) or DNA mismatch repair deficiency (dMMR). Tumors that have MSI-H or dMMR have difficulty repairing damage to their DNA. This means that they develop many mutations or changes. These changes make abnormal proteins on the tumor cells that make it easier for immune cells to find and attack the tumor.
-
NTRK gene fusions. This is a specific genetic change found in a range of cancers, including breast cancer.
-
PI3KCA gene mutation. This is a specific genetic change commonly found in breast cancer.
-
People with recurrent breast cancer sometimes experience emotions such as disbelief or fear. You are encouraged to talk with your health care team about these feelings and ask about support services to help you cope. Learn more about dealing with cancer recurrence .
Treatment options for a local or regional breast cancer recurrence
A local or regional recurrence is often manageable and may be curable. The treatment options are explained below:
-
For people with a local recurrence in the breast after initial treatment with lumpectomy and adjuvant radiation therapy, the recommended treatment is usually a mastectomy. The cancer is usually completely removed with this treatment.
-
For people with a local or regional recurrence in the chest wall after an initial mastectomy, surgical removal of the recurrence followed by radiation therapy to the chest wall and lymph nodes is the recommended treatment. However, if radiation therapy has already been given for the initial cancer, this may not be an option. Radiation therapy cannot usually be given at full dose to the same area more than once. Sometimes, systemic therapy is given before surgery to shrink the cancer and make it easier to remove.
-
Other treatments used to reduce the chance of a future distant recurrence include radiation therapy, chemotherapy, hormonal therapy, and targeted therapy. These are used depending on the tumor and the type of treatment previously received.
Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects. Your doctor may suggest clinical trials that are studying new ways to treat recurrent breast cancer.
Return to top
The next section in this guide is About Clinical Trials . It offers more information about research studies that are focused on finding better ways to care for people with breast cancer. Use the menu to choose a different section to read in this guide.
Breast Cancer - About Clinical Trials
ON THIS PAGE: You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for people with breast cancer. To make scientific advances, doctors design research studies involving volunteers, called clinical trials. Every drug that is now approved by the U.S. Food and Drug Administration (FDA) was tested in clinical trials.
Clinical trials are used for all types and stages of breast cancer. Often, clinical trials are the best option to treat breast cancer. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment.
People who participate in clinical trials can be some of the first to get a treatment before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. People are encouraged to talk with their health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a long time after treatment. Talk with your doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because no standard treatments are perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating early-stage and locally advanced breast cancer. Even if they do not benefit directly from the clinical trial, their participation may benefit future people with breast cancer. For example, the benefits of using dose-dense chemotherapy, which is giving the drugs more frequently than the traditional 3-week intervals, and adding trastuzumab for early-stage breast cancer were tested and confirmed in clinical trials.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about
health insurance coverage of clinical trials
.
Sometimes people have concerns that, in a clinical trial, they may receive no treatment by being given a placebo or a “sugar pill.” Breast cancer trials never use a placebo instead of standard treatment. Most often in a breast cancer treatment clinical trial, you will receive either the new treatment or the standard treatment. So even if you do not get the new drug or other new therapy, your breast cancer will be treated the same as if you were not in the trial. Sometimes, you may get the standard treatment plus a placebo rather than the standard treatment plus the new treatment being studied. Study participants will always be told when a placebo is used in a study. Find out more about
placebos in cancer clinical trials.
Patient safety and informed consent
To join a clinical trial, people must participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options, so that the person understands the standard treatment and how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different from the risks of standard treatment.
-
Explain what will be required of each person to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.
-
Describe the purposes of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. You will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time for personal or medical reasons, including if the new treatment is not working or if there are serious side effects. Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if they choose to leave the clinical trial before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all types of cancer. For specific topics being studied for early-stage and locally advanced breast cancer, learn more in the Latest Research section. Talking with your doctor is a good way to learn more about research opportunities in your area.
Cancer.Net offers more information about cancer clinical trials in other areas of the website, including a complete section on clinical trials and places to search for clinical trials for a specific type of cancer .
In addition, you can find a free video-based educational program about cancer clinical trials in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for breast cancer. Use the menu to choose a different section to read in this guide.
Breast Cancer - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about this type of cancer and how to treat it. Use the menu to see other pages.
Doctors are working to learn more about early-stage and locally advanced breast cancer, including ways to prevent it, how to best treat it, and how to provide the best care to people diagnosed with this disease. The following areas of research may include new options for patients through clinical trials. Always talk with your doctor about the best diagnostic and treatment options for you. Areas of research include:
-
Learning the causes of early-stage and locally advanced breast cancer, such as endocrine (hormone) disruptors, environmental causes, diet, and lifestyle choices, to find other ways to help prevent the disease.
-
Identifying new ways to prevent early-stage and locally advanced breast cancer and to help find breast cancer when it is small.
-
Developing ways to best evaluate the genes and proteins at work in each patient and each breast cancer to determine the best treatment options for each person.
-
Exploring if ductal carcinoma in situ (DCIS) should always be removed with surgery when found.
-
Determining what molecular subtypes of cancer may or may not need chemotherapy.
-
Determining the best strategies to select type and duration of adjuvant hormonal therapy.
-
Evaluating the best methods for surgery, including best management of the breast and axillary lymph nodes.
-
Testing shorter radiation therapy schedules and more targeted radiation therapy approaches.
-
Finding new reconstructive surgery approaches.
-
Testing new drug therapies and combinations of therapies for early-stage and locally advanced breast cancer, including strategies to improve hormonal therapies for ER-positive breast cancer, methods to better target the HER2 receptor for HER2-positive breast cancer, methods to best treat triple-negative breast cancer, and the use of T-DM1 for early-stage breast cancer.
-
Determining the best time to offer fertility-preserving methods.
-
Finding better ways of reducing symptoms and side effects of breast cancer treatments to improve comfort and quality of life for patients.
-
Learning more about the social and emotional factors that may affect treatment planning and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in early-stage and locally advanced breast cancer, explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your doctor or search online clinical trial databases .
-
Visit the Cancer.Net Blog to review research, information, and news about breast cancer, including perspectives from survivors.
-
Listen to a podcast from an ASCO expert discussing breast cancer research highlights from scientific meetings held in December 2022 , June 2022 , December 2021 , and June 2021 .
-
Visit the website of Conquer Cancer, the ASCO Foundation , to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance on how to cope with the physical, emotional, social, and financial changes that cancer and its treatment can bring. Use the menu to choose a different section to read in this guide.
Breast Cancer - Coping with Treatment
ON THIS PAGE: You will learn more about coping with the physical, emotional, social, and financial effects of cancer and its treatment. Use the menu to see other pages.
Every cancer treatment can cause side effects or changes to your body and how you feel. For many reasons, people do not experience the same side effects even when they are given the same treatment for the same type of cancer. This can make it hard to predict how you will feel during treatment.
As you prepare to start cancer treatment, it is normal to fear treatment-related side effects . It may help to know that your health care team will work to prevent and relieve side effects. This part of cancer treatment is called palliative care or supportive care. It is an important part of your treatment plan, regardless of your age or the stage of disease.
Coping with physical side effects
Common physical side effects from each treatment option for early-stage and locally advanced breast cancer are described in the Types of Treatment section. Learn more about side effects of cancer and its treatment, along with ways to prevent or control them . Changes to your physical health depend on several factors, including the cancer’s stage, the length and dose of treatment, and your general health.
Talk with your health care team regularly about how you are feeling. It is important to let them know about any new side effects or changes in existing side effects. If they know how you are feeling, they can find ways to relieve or manage your side effects to help you feel more comfortable and potentially keep any side effects from worsening.
You may find it helpful to keep track of your side effects so it is easier to talk about any changes with your health care team. Learn more about why tracking side effects is helpful .
Sometimes, side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment are called late effects . Treating long-term side effects and late effects is an important part of survivorship care. Learn more by reading the Follow-Up Care and Monitoring section of this guide or talking with your doctor.
Coping with emotional and social effects
You can have emotional and social effects after a cancer diagnosis. This may include dealing with a variety of emotions, such as sadness, anxiety, or anger, or managing your stress level. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about cancer.
You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your needs.
Coping with the costs of cancer care
Cancer treatment can be expensive. It may be a source of stress and anxiety for people with cancer and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their cancer treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Coping with barriers to care
Some groups of people experience different rates of new cancer cases and experience different outcomes from their cancer diagnosis. These differences are called “cancer disparities.” Disparities are caused in part by real-world barriers to quality medical care and social determinants of health , such as where a person lives and whether they have access to food and health care. Cancer disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , adults age 65+ , and people who live in rural areas or other underserved communities .
If you are having difficulty getting the care you need, talk with a member of your health care team or explore other resources that help support medically underserved people .
Talking with your health care team about side effects
Before starting treatment, talk with your doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should we call about side effects?
Be sure to tell your health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are serious. This discussion should include physical, emotional, social, and financial effects of cancer.
Caring for a loved one with cancer
Family members and friends often play an important role in taking care of a person with early-stage and locally advanced breast cancer. This is called being a caregiver. Caregivers can provide physical, practical, and emotional support to the patient, even if they live far away. Being a caregiver can also be stressful and emotionally challenging. One of the most important tasks for caregivers is
caring for themselves
.
Caregivers may have a range of responsibilities on a daily or as-needed basis, including:
-
Providing support and encouragement
-
Talking with the health care team
-
Giving medications
-
Helping manage symptoms and side effects
-
Coordinating medical appointments
-
Providing a ride to and from appointments
-
Assisting with meals
-
Helping with household chores
-
Handling insurance and billing issues
A caregiving plan can help caregivers stay organized and help identify opportunities to delegate tasks to others. It may be helpful to ask the health care team how much care will be needed at home and with daily tasks during and after treatment. Use this 1-page fact sheet to help make a caregiving action plan. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of your symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Managing Pain: Get this 32-page booklet about the importance of pain relief that includes a pain tracking sheet to help patients record how pain affects them. The free booklet is available as a PDF, so it is easy to print.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on anxiety and depression , constipation , diarrhea , rash , and immunotherapy side effects that provide a tracking sheet to record details about the side effect. These free fact sheets are available as a PDF, so they are easy to print, fill out, and give to your health care team.
The next section in this guide is Follow-Up Care and Monitoring . It explains the importance of check-ups after you finish cancer treatment. Use the menu to choose a different section to read in this guide.
Breast Cancer - Follow-Up Care and Monitoring
ON THIS PAGE: You will read about your medical care after cancer treatment for early-stage and locally advanced breast cancer is completed and why this follow-up care is important. Use the menu to see other pages.
Care for people diagnosed with cancer does not end when active treatment has finished. Your health care team will continue to check that the cancer has not come back, manage any side effects, and monitor your overall health. This is called follow-up care.
Your follow-up care may include regular physical examinations, medical tests, or both. Doctors want to keep track of your recovery in the months and years ahead. Annual mammography and physical exams are recommended surveillance strategies for people who have been treated for curable breast cancer. More intensive follow-up in people with no symptoms has not been proven to improve outcomes. However, each person should discuss with their doctor what their recommended surveillance plan is.
Breast cancer can come back, or recur, in the breast or other areas of the body. Generally, a recurrence is found when a person has symptoms that last longer than 2 weeks or an abnormal finding during a physical examination. The symptoms and signs depend on where the cancer has recurred and may include:
-
A lump under the arm or along the chest wall
-
Pain that is constant, worsening, and not relieved by over-the-counter medication, such as nonsteroidal anti-inflammatory medications (NSAIDs)
-
Bone, back, neck, or joint pain, fractures, or swelling, which can be signs of bone metastases
-
Headaches, seizures, dizziness, confusion, personality changes, loss of balance, nausea, vomiting, or changes in vision, which are possible signs of brain metastases
-
Chronic coughing, shortness of breath, or trouble breathing, which are possible symptoms of lung metastases
-
Abdominal pain, itchy skin or rash, or yellow skin and eyes from a condition called jaundice, which may be associated with liver metastases
-
Changes in energy levels, such as feeling ill or extremely tired
-
Having a low appetite and/or weight loss
-
Nausea or vomiting
-
Rash or skin changes on the breast or chest wall
-
Changes in the shape or size of the breast, or swelling in the breast or arm
However, these symptoms and signs may not always mean the cancer has returned.
It is important that your surgeon explain what your breast will feel like after surgery and, when used, radiation therapy. Over time, the breast will soften and change. But knowing what your breast will feel like can help you understand what is “normal” and what is not. If you have any questions or concerns about a symptom, you should talk with your doctor.
Follow-up care is also important for screening for other types of cancer. In some instances, patients may be able to visit a survivorship clinic that specializes in the post-treatment needs of people diagnosed with breast cancer.
Cancer rehabilitation may be recommended, and this could mean any of a wide range of services, such as physical therapy, occupational therapy, career counseling, neurocognitive testing, pain management, nutritional planning, and/or emotional counseling. The goal of rehabilitation is to help people regain control over many aspects of their lives and remain as independent as possible. Learn more about cancer rehabilitation .
Learn more about the importance of follow-up care .
Surveillance and monitoring for signs and symptoms of recurrence
One goal of follow-up care is to check for a recurrence, which means that the cancer has come back. Treatment for early-stage or locally advanced breast cancer is given to get rid of as many cancer cells in the body as possible. However, cancer recurs because small areas of cancer cells that don't respond to treatment may remain undetected in the body. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms.
Many survivors feel worried or anxious that the cancer will come back after treatment. While it often does not, it’s important to talk with your doctor about the possibility of the cancer returning. Most breast cancer recurrences are found by patients between doctor visits. The American Society of Clinical Oncology (ASCO) does not recommend routine screening for cancer at distant sites.
During follow-up care, a doctor familiar with your medical history can give you personalized information about your risk of recurrence. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the cancer does return and will help you make decisions about your treatment. Learn more about coping with the fear of recurrence .
Your doctor will ask specific questions about your health at your follow-up care appointments. Regular follow-up care recommendations depend on several factors, including the type and stage of cancer first diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results may add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects
Most people expect to have side effects when receiving treatment. However, it is often surprising to survivors that some side effects may linger beyond the treatment period. These are called long-term side effects. Other side effects called late effects may develop months or even years after treatment has ended. Long-term and late effects can include both physical and emotional changes.
Talk with your doctor about your risk of developing such side effects based on your diagnosis, your individual treatment plan, and your overall health. If you had a treatment known to cause specific late effects, you may have certain physical examinations, scans, or blood tests as part of your follow-up care to help find and manage them.
-
Long-term effects of surgery. After a mastectomy or lumpectomy to treat early-stage or locally advanced breast cancer, the breast may be scarred and may have a different shape or size than before surgery. Or, the area around the surgical site may become hardened. If lymph nodes were removed as part of the surgery or affected during treatment, lymphedema in the arm, chest wall, or breast may occur, even many years after treatment. This is a life-long risk for survivors.
-
Long-term effects of radiation therapy. Radiation therapy can also cause long-term changes to the breast, including firmness and a darker skin color. Some survivors experience breathlessness, a dry cough, and/or chest pain 2 to 3 months after finishing radiation therapy. That is because radiation therapy can cause swelling and a hardening or thickening of the lungs called fibrosis. These symptoms may seem similar to the symptoms of pneumonia but do not go away with antibiotics. The symptoms can be treated with medications called steroids. Most people fully recover with treatment. Talk with your doctor if you develop any new symptoms after radiation therapy or if the side effects are not going away.
-
Long-term effects of trastuzumab and/or chemotherapy. People who received trastuzumab or certain types of chemotherapy called anthracyclines may be at risk of heart problems. Talk with your doctor about the best ways to check for heart problems . Patients treated with chemotherapy also have a risk of other long-term side effects, such as menopausal symptoms, fatigue, chemobrain, permanent numbness and tingling of the fingers and toes, and weight gain.
-
Long-term effects of hormonal therapy. People taking tamoxifen should have yearly pelvic exams, as this drug can slightly increase the risk of uterine cancer. This risk increases with the duration of administration of tamoxifen and the age of the patient. Tell your doctor or nurse if you notice any abnormal vaginal bleeding or other new symptoms, as you may need additional tests to learn more about the cause. People who are taking an aromatase inhibitor (AI), such as anastrozole, exemestane, or letrozole, should have a bone density test periodically during treatment, as these drugs may cause some bone weakness or bone loss. Learn more about hormone therapy side effects .
In addition, people recovering from early-stage or locally advanced breast cancer can have other side effects that may continue after treatment. However, these can often be managed with medications or other options. People recovering from early-stage or locally advanced breast cancer may also experience the following long-term effects :
-
Menopausal symptoms, such as hot flashes
-
Joint pain
-
Fatigue
-
Mood changes
-
Numbness and tingling of the extremities
Vaginal dryness and a lowered sex drive are also common side effects during or after treatment for early-stage and locally advanced breast cancer. Talk with your doctor about these or other sexual health concerns . Treatment is individualized for the patient and the type of cancer and may be best managed by a gynecologist working with your oncologist.
Keeping personal health records
You and your doctor should work together to develop a personalized follow-up care plan. Be sure to discuss any concerns you have about your future physical or emotional health. ASCO offers forms to help keep track of the cancer treatment you received and develop a survivorship care plan when treatment is completed. At the conclusion of active treatment, ask your doctor to provide you with a treatment summary and a survivorship care plan.
This is also a good time to talk with your doctor about who will lead your follow-up care. Some survivors continue to see their oncologist, while others transition back to the care of their primary care doctor, another health care professional, or a specialized survivorship clinic. This decision depends on several factors, including the type and stage of cancer, side effects, health insurance rules, and your personal preferences.
If a doctor who was not directly involved in your cancer care will lead your follow-up care, be sure to share your cancer treatment summary and survivorship care plan forms with them and with all future health care providers. Details about your cancer treatment are very valuable to the health care professionals who will care for you throughout your lifetime.
The next section in this guide is Survivorship . It describes how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to choose a different section to read in this guide.
Breast Cancer - Survivorship
ON THIS PAGE: You will read about how to cope with challenges in everyday life after a cancer diagnosis. Use the menu to see other pages.
What is survivorship?
The word “survivorship” is complicated because it means different things to different people. Common definitions include:
-
Having no signs of cancer after finishing treatment.
-
Living with, through, and beyond cancer. According to this definition, cancer survivorship begins at diagnosis and continues during treatment and through the rest of a person’s life.
For some, even the term “survivorship” does not feel right, and they prefer to use different language to describe and define their experience. Sometimes extended treatment will be used for months or years to manage or control cancer. Living with cancer indefinitely is not easy, and the health care team can help you manage the
challenges that come with it
. Everyone has to find their own path to name and navigate the changes and challenges that are the results of their cancer diagnosis and treatment.
Survivors may experience a mixture of feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after a cancer diagnosis and have gained a greater acceptance of themselves. Some people may prefer to put the experience behind them and feel that their lives have not changed in a major way. Others become very anxious about their health and are uncertain about coping with everyday life. Feelings of fear and anxiety may still occur as time passes, but these emotions should not be a constant part of your daily life. If they persist, be sure to talk with a member of your health care team.
Survivors may feel some stress when their frequent visits to the health care team end after completing treatment. Often, relationships built with the cancer care team provide a sense of security during treatment, and people miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, emotional challenges such as fear of recurrence, sexual health and fertility concerns , and financial and workplace issues.
Every survivor has individual concerns and challenges. With any challenge, a good first step is being able to recognize your fears and talk about them. Effective coping requires:
-
Understanding the challenge you are facing
-
Thinking through solutions
-
Asking for and allowing the support of others
-
Feeling comfortable with the course of action you choose
Many survivors find it helpful to join an in-person support group or an online community of survivors. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of your health care team, individual counseling, or asking for assistance at the learning resource center of the place where you received treatment.
A new perspective on your health
For many people, survivorship serves as a strong motivator to make lifestyle changes.
People recovering from early-stage and locally advanced breast cancer are encouraged to follow established guidelines for good health, such as not smoking, limiting alcohol, eating well, exercising regularly, managing stress, and reaching and maintaining a healthy weight. Regular physical activity can help rebuild your strength and energy level. Your health care team can help you create an appropriate exercise plan based upon your needs, physical abilities, and fitness level. Many people find it easier to stick with an exercise program with a partner. Consider asking your spouse/partner or a friend to join you. Learn more about
making healthy lifestyle choices
.
It is important to have recommended medical checkups and tests (see
Follow-Up Care and Monitoring
) to take care of your health.
Talk with your health care team to develop a survivorship care plan that is best for your needs.
Changing role of caregivers
Family members and friends may also go through periods of transition. A caregiver plays a very important role in supporting a person diagnosed with cancer, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to the cancer diagnosis will become much less or come to an end. Caregivers can learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about cancer survivorship, explore these related items. Please note that these links will take you to other sections of Cancer.Net:
-
ASCO Answers Guide to Cancer Survivorship: Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. The free booklet is available as a PDF, so it is easy to print.
-
Survivorship Resources: Cancer.Net offers information and resources to help survivors cope, including specific sections for children , teens and young adults , and people over age 65 . There is also a main section on survivorship for people of all ages.
The next section offers Questions to Ask the Health Care Team to help start conversations with your cancer care team. Use the menu to choose a different section to read in this guide.
Breast Cancer - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask your doctor or other members of the health care team, to help you better understand your diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your health care. These suggested questions are a starting point to help you learn more about your cancer care and treatment. You are also encouraged to ask additional questions that are important to you. You may want to print this list and bring it to your next appointment. You can also download Cancer.Net’s free mobile app for a digital list and other interactive tools to manage your care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask after getting a diagnosis
-
Is there enough information to recommend a treatment plan for me? If not, which tests or procedures will be needed? Will I need to see other doctors?
-
What are my treatment plan options?
-
What treatment plan do you recommend? Why?
-
Whom would you recommend for a second opinion?
-
When do I need to make a treatment decision?
-
Who will be part of my health care team, and what does each member do?
-
Who will lead my overall treatment?
-
What is the goal of each treatment? Is it to eliminate the cancer, help me feel better, or both?
-
What can I do to get ready for treatment?
-
If I am worried about managing the costs of cancer care, who can help me? Who can help me understand what aspects of my care are covered by my insurance?
-
If I have questions or problems, who should I call?
-
Do you communicate with your patients by email or with an electronic health record system?
-
If have a strong family history of cancer, what is my chance of getting another cancer? How does that change my treatment options?
-
Should I see a genetic counselor?
-
Do you have a social worker I can speak with?
-
What should I tell my employer about my diagnosis, if anything, and what laws protect my rights as an employee?
Questions to ask your breast surgeon before your first surgery
-
Are you board-certified?
-
Do you specialize in this type of surgery?
-
How many operations like the one I am considering have you performed?
-
Do I need any other tests before this surgery?
-
Am I a candidate for a lumpectomy?
-
Do I need a mastectomy? Is reconstruction (plastic surgery) an option for me? What are the advantages and disadvantages? Is it possible to avoid removing my nipple and areola?
-
Do the lymph nodes in my underarm need to be removed?
-
What is a sentinel lymph node biopsy? What are the benefits and risks? Would you recommend it for me?
-
What is the risk of lymphedema with a sentinel lymph node biopsy? With axillary lymph node dissection?
-
What is the benefit of having more lymph nodes removed?
-
What are the side effects of these procedures? Can they be prevented or minimized?
-
Should I consider chemotherapy before surgery?
-
Will I need radiation therapy after surgery? Does this affect my reconstruction options?
-
When do I need to make a decision about surgery?
-
What should I do to get ready for the operation? Do you have recommendations on how to help me relax before surgery?
-
What medications and supplements should I stop taking? Should I stop taking hormone replacement therapy? What about birth control pills?
-
Will you describe exactly what you will do during this operation, and why?
-
Will my tumor be saved? Where will it be stored? For how long? How can it be accessed in the future?
-
What are the potential risks and side effects of this operation? What can be done to ease side effects following surgery?
-
Does the hospital offer programs that help aid healing?
-
What can I expect regarding the operation?
-
Will I need to be admitted to a hospital for this operation? If so, how long will I stay in the hospital?
-
How long will my surgery take?
-
What type of anesthesia will I need for this operation?
-
How long do I have to wait for my preoperative test results? Do I call you, or does your office call me?
-
Will a pathologist examine the tissue and write a report? Who will explain that report to me?
-
What are the possible complications for this type of surgery? How would I know if there is a problem?
-
How long will it take me to recover after the surgery?
-
When can I return to work and other daily activities?
-
Will I have stitches, staples, and/or bandages?
-
Will there be permanent effects from the surgery?
-
Where will the scar be, and what will it look like?
-
What type of clothes should I bring to go home in? Will I need a special type of bra?
-
Are there instructions or post-operative care pamphlets I can take home with me? When can I shower or bathe?
-
Will I need to have surgical drains? What does this mean? How long will the surgical drains be in?
-
Do I need a nurse to visit my home after surgery? How is this arranged?
-
When will I need to return for a follow-up appointment?
-
Will I need help at home after the surgery?
-
What kind of pain will I likely be in afterwards? Can you help me manage my pain?
-
How soon should I call your office if I experience any side effects?
Questions to ask your breast surgeon after your first surgery
-
What type of breast cancer do I have?
-
What is the size of the tumor?
-
What is the grade and stage of this disease? What are my biomarkers? What do these mean?
-
What are the chances that the breast cancer will return?
-
Can you explain my pathology report (laboratory test results) to me?
-
Can I get a copy of my pathology report? How and when can I get these results?
-
Was all of the cancer removed during the surgery?
-
Will I need to take further medication after surgery even if all of the cancer was removed? If so, why?
-
How many lymph nodes were removed?
-
Has the cancer spread to any of the lymph nodes? If so, how many? Has the cancer spread to anywhere else in my body?
-
Do I need additional surgery?
-
If I have a mastectomy without reconstruction, where can I get a prosthesis? Is this covered by my insurance?
-
Will my arm be affected by surgery? For how long? Will I need physical therapy for my arm?
-
When will I be able to work and/or return to my normal routine? Are there any activities I should avoid?
-
Who should I contact about any side effects I experience? And how soon?
-
Will my surgeon communicate with my medical oncologist or radiation oncologist?
-
Do you recommend any genetic testing of the tumor?
Questions to ask your medical oncologist
-
What is the hormone status of my tumor? What does this mean?
-
What is my HER2 status? What does this mean?
-
Do you recommend any genomic testing of the tumor? What about tests to predict the risk of recurrence? If so, which one and why?
-
What do the results of these tests mean?
-
Do you share electronic records with my surgeon?
-
Do I need more tests to find out if there is cancer anywhere else in my body?
-
Do you recommend genetic testing and seeing a genetic counselor?
-
Do I need other treatment, such as chemotherapy or hormonal therapy?
-
What is chemotherapy? What is hormonal (endocrine) therapy? What is targeted therapy? What is immunotherapy?
-
What are my treatment options?
-
What clinical trials are available for me? Where are they located, and how do I find out more about them?
-
How will each treatment option benefit me? What are the risks?
-
What is the expected timeline for each treatment option?
-
What treatment plan do you recommend for me? Why?
-
When do I need to make a decision about starting additional treatment?
-
Should I consider my family’s history of breast cancer in making my decision about treatment?
-
How does having reached (or not reached) menopause affect my treatment options?
-
What is my prognosis?
-
What can I do to get ready for this treatment?
-
Should I bring someone with me to my chemotherapy treatment?
-
What are the potential long-term or late side effects of each treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
Will I lose my hair, and can I do anything to prevent hair loss?
-
What can be done to prevent or relieve side effects?
-
How will this treatment affect my daily life? Will I be able to work, exercise, and perform my usual activities?
-
Will this treatment affect my sex life? If so, how and for how long? Is there anything I can do to prevent or treat these effects?
-
Will this treatment affect my ability to have children (fertility)? Should I talk with a fertility specialist before treatment begins? Are there other treatments available that do not pose as high a risk to my fertility but are equally effective?
-
How much time do I have before I have to start additional treatment?
-
Can I become pregnant while receiving chemotherapy or radiation therapy? What happens if I become pregnant during treatment? Is there a risk of birth defects and/or harm to the fetus and/or to me?
-
How long should I wait after cancer treatment before trying to have a child?
-
What lifestyle changes should I consider making during my treatment?
-
Do you recommend any nutritional supplements or changes to my diet?
-
Is there any risk if I take herbal supplements during my treatment?
-
If I have a strong family history of cancer, what is my chance of getting another cancer?
Questions to ask your radiation oncologist
-
What is the goal of this treatment? Is it to eliminate the cancer?
-
What are the chances that this treatment will prevent the cancer from coming back?
-
If the cancer comes back, can I get radiation therapy again?
-
How often will I receive radiation therapy?
-
Are there alternatives to the recommended treatment?
-
How much time will each treatment take?
-
Can I bring someone with me to treatment?
-
Will each treatment be the same? Does the radiation dose or area treated change throughout the period of treatment?
-
What can I do to get ready for this treatment? Are there recommendations on what clothes to wear or leave behind?
-
How will this treatment affect my daily life? Will I be able to work, exercise, and perform my usual activities?
-
Will you describe what I will experience when I receive radiation therapy? Will it hurt or cause me discomfort during the treatment?
-
What are the potential long-term or late side effects of this treatment?
-
How can I prevent or relieve those side effects?
-
Who should I contact about any side effects I experience? And how soon?
-
How will my skin be affected during radiation therapy? What skin products can I use each day?
-
Do I need to be concerned about sun exposure?
-
Should I avoid certain foods, vitamins, or supplements?
-
Should I avoid using deodorant or antiperspirant during treatment?
-
What are the possible long-term effects of this treatment?
-
If I decide to have reconstructive surgery, how would that affect my treatment plan?
-
Will this treatment affect my fertility?
-
Are there special services for patients receiving radiation therapy, such as certain parking spaces or parking rates?
Questions to ask your plastic surgeon
-
Are you board-certified? Is breast reconstruction your specialty?
-
How many breast reconstruction surgeries do you perform in a year?
-
What should I consider before deciding to have breast reconstruction?
-
What types of breast reconstruction options are available to me?
-
What are the advantages and disadvantages of each type?
-
When can I have my reconstruction?
-
Will I need surgery to the non-reconstructed breast to make the breasts match?
-
Will I need to coordinate this with my breast surgeon?
-
If I have radiation therapy, does that change my options for reconstruction?
-
What are tissue expanders, and will I need them?
-
What are the advantages and disadvantages of each reconstruction option? Does it matter if I sleep on my stomach? Will it be uncomfortable?
-
Which type of implants do you recommend (saline or silicone), and why? What size?
-
If you use tissue from another part of my body to rebuild my breast(s), where do you recommend it be taken from, and why?
-
If I have a mastectomy with implant reconstruction, can I also have a nipple reconstruction? If so, when?
-
What are the costs involved with breast reconstruction? What is covered by my insurance? Is surgery on the non-reconstructed breast covered by insurance?
-
How long will the surgery take?
-
What do I need to do to prepare for the surgery?
-
What type of anesthesia will I need for this operation?
-
What can I expect after the operation?
-
How long will I stay in the hospital?
-
What are the possible complications for this type of surgery?
-
How long will it take me to recover?
-
When can I resume my normal activities, including exercise?
-
Will I need to have surgical drains? What does this mean?
-
Will I have stitches, staples, and/or bandages?
-
Will there be a scar or other permanent effects from the surgery?
-
Are there instructions or post-operative care pamphlets I can take home with me?
-
When will I need to return for a follow-up appointment?
-
What type of results can I expect?
-
Are there photographs of reconstructed breasts that I can view?
-
How will the reconstructed breast feel to the touch?
-
What type of feeling will the reconstructed breast have?
-
What changes to the reconstructed breast can I expect over time?
-
Will I need to have surgery again in the future (for example, to replace implants over time)?
-
Do I need mammograms or magnetic resonance imaging (MRI) tests after a breast reconstruction?
-
What can I expect if my weight changes?
Questions to ask your fertility specialist
If you are concerned about your ability to have children in the future, you are encouraged to talk with a fertility specialist (in addition to the doctors listed above). You should have this discussion as soon as possible after your diagnosis and before cancer treatment begins. Recommendations from the fertility specialist should always be discussed with your oncologist as well before starting any fertility-related efforts.
-
How often do you advise people with cancer?
-
What are my options to preserve my fertility?
-
How well does each option work?
-
What are the costs involved with my options to preserve fertility? What is covered by my insurance?
Learn more about preserving fertility before cancer treatment .
Questions to ask about planning follow-up care
-
What is the chance that the cancer will come back? Should I watch for specific signs or symptoms?
-
What long-term side effects or late effects are possible based on the cancer treatment I received?
-
After my treatment has ended, what will my follow-up care plan be?
-
How often will I need to see a doctor?
-
If I move or need to switch doctors, how do I make sure to continue my recommended follow-up care schedule?
-
What follow-up tests will I need, and how often will those tests be needed?
-
Can I get copies of my laboratory test results?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
Who will lead my follow-up care?
-
What survivorship support services are available to me? To my family?
The next section in this guide is Additional Resources . It offers more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Breast Cancer - Additional Resources
ON THIS PAGE: You will find some helpful links to other areas of Cancer.Net that provide information about cancer care and treatment. This is the final page of Cancer.Net’s Guide to Breast Cancer. Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of cancer for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment, and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Search for a cancer specialist in your local area using this free database of doctors from the American Society of Clinical Oncology (ASCO).
-
Learn what medical phrases and terms used in cancer care and treatment mean.
-
Read more about the first steps to take when you are diagnosed with cancer .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of cancer care.
-
Learn more about coping with the emotions that cancer can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for people with breast cancer.
-
Explore what to do when you finish active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
-
Watch Cancer.Net videos with ASCO experts explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
-
For more information about treatment options for this disease, see the following topic review from UpToDate: Patient information: Breast cancer guide to diagnosis and treatment (Beyond the Basics) . Please note that this link takes you to a separate, independent website.
This is the end of Cancer.Net’s Guide to Breast Cancer. Use the menu to select another section to continue reading this guide.