













Brain Tumor - Introduction
ON THIS PAGE: You will find some basic information about this disease and the parts of the body it may affect. This is the first page of Cancer.Net’s Guide to Brain Tumors. Use the menu to see other pages. Think of that menu as a roadmap for this entire guide.
The possibility of being diagnosed with a brain tumor can be a shocking and life-changing event. If your doctor suspects a brain tumor, it is important to seek out doctors who specialize in diagnosing and treating brain tumors. The brain is a complex and vital organ, and treatment often causes life-long changes. Research about brain tumor treatment is ongoing, so it is important to get updated medical information about treatment options about the specific type of brain tumor and to get specialists' opinions about your treatment plan.
About the brain and central nervous system
The brain and spinal column make up the central nervous system (CNS), where all vital functions are controlled. These functions include thought, speech, and body movements. This means that when a tumor grows in the CNS, it can affect a person's thought processes or the way they talk or move.
Anatomy of the brain
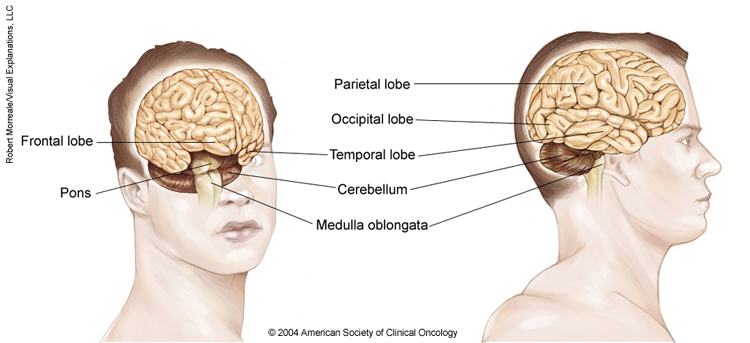
The brain is made up of 3 main parts: the cerebrum, the cerebellum, and the brain stem. The meninges, which surround the brain, are also considered part of the brain.
-
The cerebrum. This is the largest part of the brain. It contains 2 cerebral hemispheres on either side of the brain that each control the opposite side of the body. It is divided into 4 lobes where specific functions occur:
-
The frontal lobe controls reasoning, emotions, problem-solving, expressive speech, and movement.
-
The parietal lobe controls the sensations of touch, such as pressure, pain, and temperature. It also controls parts of speech, visual-spatial orientation, and calculation.
-
The temporal lobe controls memory, special senses such as hearing, and the ability to understand spoken or written words.
-
The occipital lobe controls vision.
-
-
The cerebellum. The cerebellum is located at the back part of the brain below the cerebrum. It is responsible for coordination and balance, and it controls functions on the same side of the body.
-
The brain stem. This is the portion of the brain that connects to the spinal cord and the cerebellum. It controls involuntary functions essential for life, such as the beating of the heart and breathing. Messages for the functions controlled by the cerebrum and cerebellum travel through the brain stem to the body.
-
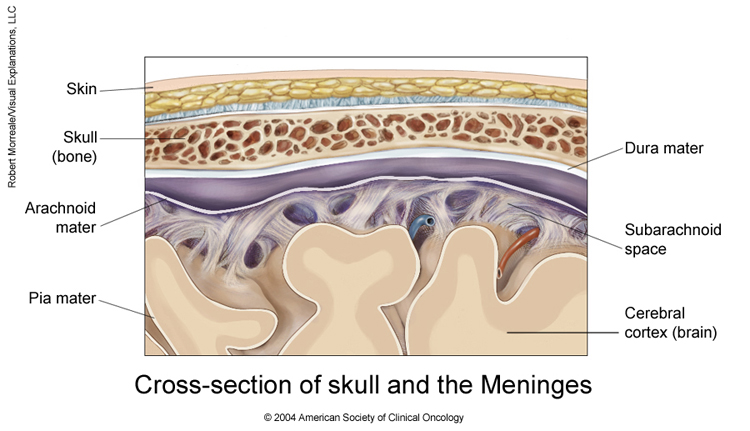
The meninges. These are the membranes that surround and protect the brain and spinal cord. There are 3 meningeal layers, called the dura mater, arachnoid, and pia mater. The cerebrospinal fluid (CSF) is made near the center of the brain, in the lateral ventricles. CSF circulates around the brain and spinal cord between the arachnoid and pia layers.
About primary brain tumors
A primary brain tumor is a tumor that starts in the brain. A primary brain tumor is often described as either "low grade" or "high grade." A low-grade tumor generally grows slowly, but it can turn into a high-grade tumor. A high-grade tumor is more likely to grow faster.
In adults, a secondary brain tumor, also called a brain metastasis, is much more common than a primary brain tumor.
About secondary brain tumors
A secondary brain tumor, or brain metastasis, is a cancerous tumor that started in another part of the body, such as the breast, lung, or colon, and then spread to the brain. A secondary brain tumor may also be called metastatic cancer. For instance, lung cancer that has spread to the brain may be called metastatic lung cancer.
If cancer spreads to the meninges and CSF, it is called leptomeningeal metastases or neoplastic meningitis. This condition occurs more commonly in people with leukemia, lymphoma, melanoma, breast cancer, or lung cancer.
The rest of this guide mainly covers primary brain tumors in adults, while providing some information on brain metastases. To learn more detailed information about cancer that started elsewhere in the body and spread to the brain, read about that specific type of cancer . Learn about brain tumors in children in a different guide on this same website.
Types of primary brain tumors in adults
There are many types of primary brain tumors. Some cannot be assigned an exact type because the tumor’s location makes it too difficult to remove for full testing.
Descriptions of more common brain tumor types in adults are described below, divided into glioma and non-glioma tumor types.
Gliomas
As a group, gliomas are one of the most common types of brain tumors. While the exact origin of gliomas is still unknown, they are thought to grow from glial cells or glial precursor cells. A glial cell is a type of supportive cell in the brain. The main types of supportive cells in the brain include astrocytes, oligodendrocytes, and ependymal cells. Gliomas may be considered astrocytoma, oligodendroglioma, or ependymoma. Gliomas are assigned a grade, which is an indication of how aggressive a tumor is likely to be. A higher grade is usually more aggressive and more likely to grow quickly. However, current research is helping doctors move toward using tumor genetics to better classify gliomas. This is discussed elsewhere in this guide. Unlike most tumors that start outside of the brain and CNS, most primary brain tumors like glioma are not assigned a "stage." For tumors that do not begin in the brain, a higher cancer "stage" number usually describes whether the primary tumor has spread to other parts of the body, and this information influences which treatments are selected. Primary brain tumors, like gliomas, only rarely spread outside of the brain. Thus, they do not need to be staged to help the clinical team decide on the appropriate treatments.
Currently, the types of gliomas include:
-
Astrocytoma. Astrocytoma is the most common type of glioma. Astrocytoma cells look like glial cells called astrocytes that are found in the cerebrum or cerebellum. Historically, there have been 4 grades of astrocytoma, which are described below.
-
Grade 1 or pilocytic astrocytoma is a slow-growing tumor that is most often benign and rarely spreads into nearby tissue. Benign means the tumor can grow but does not spread to other parts of the body.
-
Grade 2 astrocytoma is a slow-growing malignant tumor that can often spread into nearby tissue and can become a higher grade. Malignant means it is cancerous and can spread to other parts of the body.
-
Grade 3 or anaplastic astrocytoma is a malignant tumor that can quickly grow and spread to nearby tissues.
-
Grade 4 or glioblastoma is a very aggressive form of astrocytoma.
A new international classification system for primary brain tumors was unveiled by the World Health Organization (WHO) in 2021. This system divides astrocytomas and other types of brain tumors into many subgroups depending largely on their genetic makeup and the presence or absence of certain important changes in the tumor's specific genes. The treatment team will use information from an analysis of each tumor sample to precisely classify each tumor using the new guidelines. (Learn more about biomarker testing of the tumor in the Diagnosis section.) Key changes for the most common types of astrocytomas include:
-
Adult diffuse astrocytomas have now been grouped based on whether there is a mutation in the isocitrate dehydrogenase ( IDH ) gene. There are 2 groups: 1 ) astrocytoma, IDH mutant, and 2 ) glioblastoma, IDH wild-type. "Wild-type" means that the gene is found in its natural, unmutated form.
-
Astrocytoma, IDH mutant, can be a grade 2, grade 3, or grade 4 tumor, based on whether there are other genetic and tumor features, including a high rate of cell division (called the mitotic index) and alterations in the CDKN2A/B genes. These were previously called IDH -mutant or secondary glioblastomas.
-
Glioblastoma is now only used to describe IDH wild-type tumors that also have 1 or more of the following features: loss of chromosome 10, gain of chromosome 7, TERT promoter mutation, and increased number of copies of the EGFR gene. Unlike the previous classification system, glioblastomas are do not also have to show signs of cell death and excessive growth of blood vessels.
-
-
Oligodendroglioma. Oligodendroglioma is a tumor whose cells look like glial cells called oligodendrocytes. These cells are responsible for making myelin. Myelin surrounds the nerves and is rich in protein and fatty substances called lipids. Under the 2021 WHO guidelines, these tumors must have an IDH mutation and contain a chromosome 1p and 19q codeletion. They are categorized as either grade 2 oligodendroglioma, which is considered low grade, or grade 3 oligodendroglioma, which is considered a high-grade tumor with anaplastic features.
-
Ependymoma. Ependymoma commonly begins in the passageways in the brain where CSF is made and stored. In adults, they occur more often in the spine and can also be of the myxopapillary subtype. Learn about ependymoma in children .
-
Diffuse midline glioma. A diffuse midline glioma begins in the glial cells in the brain stem, spinal cord, and other midline structures within the CNS. Learn about brain stem glioma in children .
Non-glioma tumors
Non-glioma tumors are tumors that arise from cells in the brain that are not glial cells. Types of non-glioma tumors include:
-
Meningioma. Meningioma is the most common primary brain tumor. It begins in the meninges and is most often noncancerous. Meningioma can cause serious symptoms if it grows and presses on the brain or spinal cord or grows into the brain tissue. Learn more about meningioma .
-
Pineal gland and pituitary gland tumors. These are tumors that start in the pineal gland and pituitary gland .
-
Primary CNS lymphoma . This is a form of lymphoma . Lymphoma is a cancer that begins in the lymphatic system. Primary CNS lymphoma starts in the brain and can spread to the spinal fluid and eyes.
-
Medulloblastoma. Medulloblastoma is thought to start from a specific type of cell in the cerebellum. These cells are called cerebellar granule progenitor cells. It is most common in children and is usually cancerous, often spreading throughout the CNS. Learn about medulloblastoma in children .
-
Craniopharyngioma. Craniopharyngioma is a benign tumor that begins near the pituitary gland located near the base of the brain. These tumors are uncommon. Learn about craniopharyngioma in children .
-
Schwannoma. Schwannoma is a rare tumor that begins in the nerve sheath, or the lining of the nerves. It may often occur in the vestibular nerve, which is a nerve in the inner ear that helps control balance. It is typically noncancerous.
For a complete list of all types of brain tumors and how often they are diagnosed, the website of the Central Brain Tumor Registry of the United States offers this information in its reports. (Please note that this link takes you to another organization's website.)
Looking for More of an Introduction?
If you would like more of an introduction, explore these related items. Please note that these links will take you to other sections on Cancer.Net:
-
Cancer.Net En Español: Read about brain tumors in Spanish. Infórmase sobre tumor cerebral en español.
-
Find a Doctor. Search for a specialist in your local area using this free database of doctors from the American Society of Clinical Oncology (ASCO).
-
Cancer Terms. Learn what medical phrases and terms used in cancer care and treatment mean.
The next section in this guide is Medical Illustrations . It offers drawings of body parts often affected by a brain tumor. Use the menu to choose a different section to read in this guide.
Brain Tumor - Medical Illustrations
ON THIS PAGE: You will find drawings of the main body parts affected by a brain tumor. Use the menu to see other pages.
The next section in this guide is Statistics . It helps explain the number of people who are diagnosed with a brain tumor and general survival rates. Use the menu to choose a different section to read in this guide.
Brain Tumor - Statistics
ON THIS PAGE: You will find information about the estimated number of people who will diagnosed with a brain tumor each year. You will also read general information on surviving the disease. Remember, survival rates depend on several factors, and no 2 people with a tumor are the same. Use the menu to see other pages.
Every person is different, with different factors influencing their risk of being diagnosed with this tumor and the chance of recovery after a diagnosis. It is important to talk with your doctor about any questions you have around the general statistics provided below and what they may mean for you individually. The original sources for these statistics are provided at the bottom of this page.
How many people are diagnosed with a brain tumor?
A primary brain or spinal cord tumor is a tumor that starts in the brain or spinal cord. In 2023, an estimated 24,810 adults (14,280 men and 10,530 women) in the United States will be diagnosed with primary cancerous tumors of the brain and spinal cord. A person’s likelihood of developing this type of tumor in their lifetime is less than 1%. Brain tumors account for 85% to 90% of all primary central nervous system (CNS) tumors. Worldwide, an estimated 308,102 people were diagnosed with a primary brain or spinal cord tumor in 2020.
It is estimated that 5,230 children under the age of 20 will also be diagnosed with a CNS tumor in the United States in 2023. The rest of this guide deals with primary brain tumors in adults. Learn more about brain tumors in children .
In addition to primary brain tumors, there are also secondary brain tumors or brain metastases. This is when the tumor started somewhere else in the body and spread to the brain. The most common cancers that spread to the brain are breast , kidney , and lung cancers, as well as leukemia, lymphoma , and melanoma . This guide covers primary adult brain tumors only.
Brain and other nervous system cancer is the 10th leading cause of death for men and women. It is estimated that 18,990 deaths (11,020 men and 7,970 women) from primary cancerous brain and CNS tumors will occur in the United States in 2023. In 2020, an estimated 251,329 people worldwide died from primary cancerous brain and CNS tumors.
What is the survival rate for a brain tumor?
There are different types of statistics that can help doctors evaluate a person’s chance of recovery from a brain tumor. These are called survival statistics. A specific type of survival statistic is called the relative survival rate. It is often used to predict how having a tumor may affect life expectancy. Relative survival rate looks at how likely people with a brain tumor are to survive for a certain amount of time after their initial diagnosis or start of treatment compared to the expected survival of similar people without this tumor.
Example:
Here is an example to help explain what a relative survival rate means. Please note this is only an example and not specific to this type of cancer. Let’s assume that the 5-year relative survival rate for a specific type of cancer is 90%. “Percent” means how many out of 100. Imagine there are 1,000 people without cancer, and based on their age and other characteristics, you expect 900 of the 1,000 to be alive in 5 years. Also imagine there are another 1,000 people similar in age and other characteristics as the first 1,000, but they all have the specific type of cancer that has a 5-year survival rate of 90%. This means it is expected that 810 of the people with the specific cancer (90% of 900) will be alive in 5 years.
It is important to remember that statistics on the survival rates for people with a brain tumor are only an estimate. They cannot tell an individual person if the tumor will or will not shorten their life. Instead, these statistics describe trends in groups of people previously diagnosed with the same disease, including specific stages of the disease.
The 5-year relative survival rate for a cancerous brain or CNS tumor is almost 36%. The 10-year survival rate is over 30%.
The survival rates for a brain tumor vary based on several factors. These include the grade and prognostic factors of a tumor, a person’s age and general health, and how well the treatment plan works. Another factor that can affect outcomes is the type of brain or spinal cord tumor ( see Introduction ).
The 5-year relative survival rate for people younger than age 15 is about 75%. For people age 15 to 39, the 5-year relative survival rate nears 72%. The 5-year relative survival rate for people age 40 and older is 21%.
Experts measure relative survival rate statistics for a brain tumor every 5 years. This means the estimate may not reflect the results of advancements in how a brain tumor is diagnosed or treated from the last 5 years. Talk with your doctor if you have any questions about this information. Learn more about understanding statistics .
Statistics adapted from the American Cancer Society's publication, Cancer Facts & Figures 2023 ; the ACS website; the CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2015-2019 , published October 2022; the International Agency for Research on Cancer website; and the National Cancer Institute website. (All sources accessed February 2023.)
The next section in this guide is Risk Factors . It describes the factors that may increase the chance of developing a brain tumor. Use the menu to choose a different section to read in this guide.
Brain Tumor - Risk Factors
ON THIS PAGE: You will find out more about the factors that increase the chance of developing a brain tumor. Use the menu to see other pages.
What are the risk factors for a brain tumor?
A risk factor is anything that increases a person’s chance of developing a brain tumor. Although risk factors often influence the development of a brain tumor, most do not directly cause a brain tumor. Some people with several risk factors never develop a brain tumor, while others with no known risk factors do. Knowing your risk factors and talking about them with your doctor may help you make more informed decisions. But, at this time, there are no known ways to prevent a brain tumor through lifestyle changes.
Most of the time, the cause of a brain tumor is unknown. However, the following factors may raise a person’s risk of developing a brain tumor:
-
Age. Brain tumors are more common in children and older adults , although people of any age can develop a brain tumor.
-
Sex. In general, men are more likely than women to develop a brain tumor. However, some specific types of brain tumors, such as meningioma, are more common in women.
-
Home and work exposures. Exposure to solvents, pesticides, oil products, rubber, or vinyl chloride may increase the risk of developing a brain tumor. However, there is not yet scientific evidence that supports this possible link.
-
Family history. About 5% of brain tumors may be linked to hereditary genetic factors or conditions, including Li-Fraumeni syndrome , neurofibromatosis , nevoid basal cell carcinoma syndrome , tuberous sclerosis , Turcot syndrome , and von Hippel-Lindau disease . Scientists have also found “clusters” of brain tumors within some families without a link to these known hereditary conditions. Studies are underway to try to find a cause for these clusters.
-
Exposure to infections, viruses, and allergens. Infection with the Epstein - Barr virus (EBV) increases the risk of central nervous system (CNS) lymphoma. EBV is more commonly known as the virus that causes mononucleosis or “mono.” In other research, high levels of a common virus called cytomegalovirus (CMV) have been found in brain tumor tissue. The meaning of this finding is being researched. Several types of other viruses have been shown to cause brain tumors in research on animals. More data are needed to find out if exposure to infections, other viruses, or allergens increase the risk of a brain tumor in people. Of note, studies have shown that patients with a history of allergies or skin conditions have a lower risk of glioma.
-
Electromagnetic fields. Most studies evaluating the role of electromagnetic fields, such as energy from power lines or from cell phone use, show no link to an increased risk of developing a brain tumor in adults. Because of conflicting information regarding risk in children, the World Health Organization (WHO) recommends limiting cell phone use and promotes the use of a hands-free headset for both adults and children.
-
Race and ethnicity. In the United States, White people are more likely to develop gliomas but less likely to develop meningioma than Black people. Also, people from northern Europe are more than twice as likely to develop a brain tumor as people in Japan.
-
Ionizing radiation. Previous treatment to the brain or head with ionizing radiation, including x-rays, has been shown to be a risk factor for a brain tumor.
-
Head injury and seizures. Serious head trauma has long been studied for its relationship to brain tumors. Some studies have shown a link between head trauma and meningioma but not between head trauma and glioma. A history of seizures has also been linked with brain tumors, but because a brain tumor can cause seizures, it is not known if seizures increase the risk of brain tumors, if seizures occur because of the tumor, or if anti-seizure medication increases the risk.
-
N-nitroso compounds. Some studies of diet and vitamin supplementation seem to indicate that dietary N-nitroso compounds may raise the risk of both childhood and adult brain tumors. Dietary N-nitroso compounds are formed in the body from nitrites or nitrates found in some cured meats, cigarette smoke, and cosmetics. However, additional research is necessary before a definitive link can be established.
The next section in this guide is Symptoms and Signs . It explains what changes or medical problems a brain tumor can cause. Use the menu to choose a different section to read in this guide.
Brain Tumor - Symptoms and Signs
ON THIS PAGE: You will find out more about the changes and medical problems that can be a sign of a brain tumor. Use the menu to see other pages.
What are the symptoms and signs of a brain tumor?
People with a brain tumor may experience one or more of the following symptoms or signs. Symptoms are changes that you can feel in your body. Signs are changes in something measured, like taking your blood pressure or doing a lab test. Together, symptoms and signs can help describe a medical problem. Sometimes, people with a brain tumor do not have any of the symptoms and signs described below. Or, the cause of a symptom or sign may be a medical condition that is not a brain tumor.
Symptoms of a brain tumor can be general or specific. A general symptom is caused by the pressure of the tumor on the brain or spinal cord. Specific symptoms are caused when a specific part of the brain is not working well because of the tumor. For many people with a brain tumor, they were diagnosed when they went to the doctor after experiencing a problem, such as a headache or other changes.
General symptoms of a brain tumor
-
Headaches, which may be severe and worsen with activity or in the early morning
-
Seizures. People may experience different types of seizures. Certain drugs can help prevent or control them. Motor seizures, also called convulsions, are sudden involuntary movements of a person’s muscles. The different types of seizures and what they look like are listed below:
-
Myoclonic
-
Single or multiple muscle twitches, jerks, spasms
-
-
Tonic-Clonic (Grand Mal)
-
Loss of consciousness and body tone, followed by twitching and relaxing muscles that are called contractions
-
Loss of control of body functions, such as loss of bladder control
-
May be a short 30-second period of no breathing and a person's skin may turn a shade of blue, purple, gray, white, or green
-
After this type of seizure, a person may be sleepy and experience a headache, confusion, weakness, numbness, and sore muscles
-
-
Sensory
-
Change in sensation, vision, smell, and/or hearing without losing consciousness
-
-
Complex partial
-
May cause a loss of awareness or a partial or total loss of consciousness
-
May be associated with repetitive, unintentional movements, such as twitching
-
-
-
Personality or memory changes
-
Nausea or vomiting
-
Fatigue
-
Drowsiness
-
Sleep problems
-
Memory problems
-
Changes in ability to walk or perform daily activities
Symptoms that may be specific to the brain tumor location
-
Pressure or headache near the tumor.
-
Loss of balance and difficulty with fine motor skills is linked with a tumor in the cerebellum.
-
Changes in judgment, including loss of initiative, sluggishness, and muscle weakness or paralysis is associated with a tumor in the frontal lobe of the cerebrum.
-
Partial or complete loss of vision is caused by a tumor in the occipital lobe or temporal lobe of the cerebrum.
-
Changes in speech, hearing, memory, or emotional state, such as aggressiveness and problems understanding or retrieving words can develop from a tumor in the frontal and temporal lobe of the cerebrum.
-
Altered perception of touch or pressure, arm or leg weakness on 1 side of the body, or confusion with left and right sides of the body are linked to a tumor in the frontal or parietal lobe of the cerebrum.
-
Inability to look upward can be caused by a pineal gland tumor.
-
Lactation, which is the secretion of breast milk, and altered menstrual periods, as well as growth of the hands and feet during adulthood, are linked with a pituitary tumor.
-
Difficulty swallowing, facial weakness or numbness, or double vision is a symptom of a tumor in the brain stem.
-
Vision changes, including loss of part of the vision or double vision can be from a tumor in the temporal lobe, occipital lobe, or brain stem.
If you are concerned about any changes you experience, please talk with your doctor. Your doctor will try to understand what is causing your symptom(s). They may do an exam and order tests to understand the cause of the problem, which is called a diagnosis.
If a brain tumor is diagnosed, relieving symptoms remains an important part of your care and treatment. Managing symptoms may also be called "palliative and supportive care," which is not the same as hospice care given at the end of life. This type of care focuses on managing symptoms and supporting people who face serious illnesses, such as cancer. You can receive palliative and supportive care at any time during cancer treatment. Learn more in this guide’s section on Coping with Treatment .
Be sure to talk with your health care team about the symptoms you experience, including any new symptoms or a change in symptoms. Learn more about managing symptoms of a brain tumor in the Types of Treatment section.
The next section in this guide is Diagnosis . It explains what tests may be needed to learn more about the cause of the symptoms. Use the menu to choose a different section to read in this guide.
Brain Tumor - Diagnosis
ON THIS PAGE: You will find a list of common tests, procedures, and scans that doctors use to find the cause of a medical problem. Use the menu to see other pages.
Doctors use many tests to find, or diagnose, a brain tumor and learn the type of brain tumor. They also do tests to find out if it has spread to another part of the body from where it started. This is called metastasis and is rare for a primary brain tumor. Doctors may also do tests to learn which treatments could work best.
For most types of tumors, taking a sample of the possible tumor is the only sure way for the doctor to know if an area of the body has a tumor. This may be done in a procedure called a biopsy or by removing part or all of the tumor with surgery. In a biopsy, the doctor takes a small sample of tissue for testing in a laboratory. If this is not possible, the doctor may suggest other tests that will help make a diagnosis.
How a brain tumor is diagnosed
Imaging tests can help doctors find out if the tumor is a primary brain tumor or if it is cancer that has spread to the brain from elsewhere in the body. Imaging tests show pictures of the inside of the body. Your doctor may consider these factors when choosing a diagnostic test:
-
The type of tumor suspected
-
Your signs and symptoms
-
Your age and general health
-
The results of earlier medical tests
Most brain tumors are diagnosed after symptoms appear. Often a brain tumor is first diagnosed by an internist or a neurologist. An internist is a doctor who specializes in treating adults. A neurologist is a doctor who specializes in problems with the brain and central nervous system (CNS).
In addition to asking the patient for a detailed medical history and doing a physical examination, the doctor may recommend the tests described below. These tests are to help find out the presence, and sometimes the type or grade, of a brain tumor.
In general, diagnosing a brain tumor usually begins with magnetic resonance imaging (MRI). Once MRI shows that there is a tumor in the brain, the most common way to determine the type of brain tumor is to look at the results from a sample of tissue after a biopsy or surgery. These tests and procedures are described below in more detail.
-
MRI. An MRI produces detailed images of the inside of the body using magnetic fields, not x-rays. MRI can be used to measure the tumor’s size. A special dye called a contrast medium is given before the scan to create a clearer picture. This dye can be injected into a patient’s vein. MRIs create more detailed pictures than computed tomography (CT) scans (see below) and are the preferred way to diagnose a brain tumor. The MRI may be of the brain, spinal cord, or both, depending on the type of tumor suspected and the likelihood that it will spread in the CNS. There are different types of MRI. The results of a neuro-examination, done by the internist or neurologist, helps determine which type of MRI to use.
-
Intravenous (IV) gadolinium-enhanced MRI is typically used to help create a clearer picture of a brain tumor. This is when a patient first has a regular MRI and afterwards is given a special type of contrast medium called gadolinium through an IV. Then, a second MRI is done to get another series of pictures using the dye.
-
An MRI technique called "diffusion weighted imaging" helps show the cellular structure of the brain. Another technique called "perfusion imaging" shows how much blood is reaching the tumor. These methods may help doctors predict how well treatment will work.
-
A spinal MRI may be used to diagnose a tumor on or near the spine.
-
A functional MRI (fMRI) provides information about the location of specific areas of the brain that are responsible for muscle movement and speech. During the fMRI examination, the patient is asked to do certain tasks that cause changes in the brain and can be seen on the fMRI image. This test is used to help plan surgery, so the surgeon can avoid damaging the functional parts of the brain while removing the tumor.
-
Magnetic resonance spectroscopy (MRS) is a test using an MRI that provides information on the chemical composition of the brain. It can help tell the difference between any dead tissue caused by previous radiation treatments and new tumor cells in the brain.
-
-
Tissue sampling/biopsy/surgical removal of a tumor. A sample of the tumor’s tissue is usually needed to make a final diagnosis. During biopsy, a small amount of tissue is removed for examination under a microscope. Biopsy is the only way to make a definite diagnosis of a brain tumor, even if other tests can suggest that cancer is present. A pathologist then analyzes the sample(s). A pathologist is a doctor who specializes in interpreting laboratory tests and evaluating cells, tissues, and organs to diagnose disease. A biopsy can be done as part of surgery to remove the entire tumor. Or surgery may be done as a separate procedure if completely removing the tumor is not possible because of its specific location in the brain or a patient’s overall health.
Your health care team may also recommend other tests to help make a diagnosis or find out how well treatment is working. Not all tests described here will be used for every person.
-
CT scan. A CT scan takes pictures of the inside of the body using x-rays taken from different angles. A computer combines these pictures into a detailed, 3-dimensional image that shows any abnormalities or tumors. A CT scan can help find bleeding and enlargement of the fluid-filled spaces in the brain, called ventricles. Changes to bone in the skull can also be seen on a CT scan, and it can be used to measure a tumor’s size. A CT scan may also be used if the patient cannot have an MRI; for example, if the person has a pacemaker for their heart. Sometimes, a contrast medium is given before the scan to provide better detail on the image. This dye can be injected into a patient’s vein and/or given as a pill or liquid to swallow.
-
Positron emission tomography (PET) or PET-CT scan. A PET scan is a way to create pictures of organs and tissues inside the body using various substances, such as sugars or proteins. A PET scan is used at first to find out more about a tumor while a patient is receiving treatment. It may also be used if the tumor comes back after treatment. A PET scan is usually combined with a CT scan (see above), called a PET-CT scan . However, you may hear your doctor refer to this procedure just as a PET scan. A small amount of a radioactive substance is injected into the patient’s body. This substance is taken up by cells that are actively dividing. Because tumor cells are more likely to be actively dividing, they absorb more of the radioactive substance. However, the amount of radiation in the substance is too low to be harmful. A scanner then detects this substance to produce images of the inside of the body.
-
Cerebral arteriogram, also called a cerebral angiogram. A cerebral arteriogram shows the arteries in the brain. It is an x-ray, or series of x-rays, of the head. X-rays are taken after a special dye called a contrast medium is injected into the main arteries of the patient’s head.
-
Lumbar puncture or spinal tap. A lumbar puncture looks for cancer cells, blood, or tumor markers in a sample of cerebrospinal fluid (CSF), which is removed using a needle. Tumor markers or biomarkers are substances found in higher-than-normal amounts in the blood, urine, spinal fluid, plasma or other bodily fluids of people with certain types of tumors. Typically, a local anesthetic is given to numb the patient’s lower back before the procedure.
-
Myelogram. The doctor may recommend a myelogram to find out if the tumor has spread to the spinal fluid, other parts of the brain, or the spinal cord. A myelogram uses a dye injected into the CSF that surrounds the spinal cord. The dye shows up on an x-ray and can outline the spinal cord to help the doctor look for a tumor. This test is only done occasionally; a lumbar puncture (see above) is more common.
-
Biomarker testing of the tumor. Your doctor may recommend running laboratory tests on a tumor sample to identify specific genes, proteins, and other factors, such as tumor markers, unique to the tumor. This may also be called molecular testing of the tumor. Some biomarkers may help doctors determine a patient’s prognosis, which is the chance of recovery (see Grades and Prognostic Factors ). Researchers are examining biomarkers to find ways to diagnose a brain tumor before symptoms begin. Results of these tests may help determine your treatment options . The markers most commonly looked at for brain tumors include:
-
For oligodendroglioma, the loss of the p-arm of chromosome 1 and the loss of the q-arm of chromosome 19. This is called a 1p/19q codeletion. It is linked to more successful treatment, particularly with chemotherapy. It can be used to help plan treatment, especially for anaplastic oligodendroglioma.
-
A mutation in the isocitrate dehydrogenase ( IDH ) gene, which is found in about 70% to 80% of low-grade gliomas in adults. Higher-grade tumors can also have IDH gene mutations, which suggests that these tumors started as lower-grade tumors that became a higher grade. This mutation is linked with a better prognosis in both low-grade and high-grade tumors.
-
In glioblastoma, whether a gene called methyl guanine methyl transferase ( MGMT) is changed can help the doctor understand a patient’s prognosis and how well treatment will work. Its role in determining the benefit of treatment is being tested in clinical trials.
-
-
Neurological, vision, and hearing tests. These tests help determine if a tumor is affecting how the brain functions. An eye examination can detect changes to the optic nerve, as well as changes to a person’s field of vision.
-
Neurocognitive assessment. This consists of a detailed evaluation of all major functions of the brain, such as storage and retrieval of memory, expressive and receptive language abilities, calculation, dexterity, and the overall well-being of the patient. These tests are done by a licensed clinical neuropsychologist. This specialist will write a formal report to compare with future evaluations or identify specific problems that can be helped through treatment.
-
Electroencephalography (EEG). An EEG is a noninvasive test in which electrodes are attached to the outside of a person's head to measure electrical activity of the brain. It is used to monitor for possible seizures (see Symptoms and Signs ).
-
Evoked potentials. Evoked potentials involve the use of electrodes to measure the electrical activity of nerves and can often detect acoustic schwannoma, a noncancerous brain tumor. This test can be used as a guide when removing a tumor that is growing around important nerves.
Test results
After diagnostic tests are done, your doctor will review the test results with you. If the diagnosis is a brain tumor, additional tests will be done to learn more about the tumor. The results help the doctor describe the tumor and plan your treatment.
The next section in this guide is Grades and Prognostic Factors . It explains the system doctors use to describe a brain tumor. Use the menu to choose a different section to read in this guide.
Brain Tumor - Grades and Prognostic Factors
ON THIS PAGE: You will learn about how doctors describe a brain tumor’s growth or spread. This is called the grade. You will also learn about the prognostic factors doctors use to help plan treatment. Use the menu to see other pages.
What is cancer staging?
For most other types of tumors in other parts of the body, a staging system is used to describe where a tumor is located, if or where it has spread, and whether it is affecting other parts of the body. However, there is no recommended systemic staging system for adult brain tumors because most primary brain tumors do not usually spread beyond the central nervous system (CNS). The grading system described below is always used instead because the specific features of a brain tumor determine how cancerous it is and how likely it is to grow.
Prognostic factors
To decide on the best treatment for a brain tumor, both the type and grade of the tumor must be determined. There are several factors that help doctors determine the appropriate brain tumor treatment plan and a patient's prognosis, which is the chance of recovery:
-
Tumor histology. As outlined in the Diagnosis section, a sample of the tumor is removed for analysis. Tumor histology includes finding out the type of tumor, the grade, and additional molecular features that predict how quickly the tumor can grow. Together, these factors will help your doctor understand how the tumor will likely behave. These factors may also help determine your treatment options.
Prior to 2021, brain tumors were defined by grades (1 to 4) based on how the tissue looked under a microscope. This grade indicated whether a tumor was growing slowly or quickly. As described in the Introduction , in 2021 the World Health Organization released a new classification and grading system that uses specific features to describe whether a tumor will grow slowly or quickly. These features include whether there is an IDH mutation, high rate of cell division (called the mitotic index), alterations in the CDKN2A/B genes, loss of chromosome 10, gain of chromosome 7, a TERT promoter mutation, and increased number of copies of the EGFR gene.
-
Age. In adults, a person’s age and level of functioning, called functional status (see below), when diagnosed is one of the best ways to predict a patient’s prognosis. In general, younger adults have a better prognosis.
-
Symptoms. The symptoms a patient has and how long they last may also help determine prognosis. For example, seizures and having symptoms for a long time are linked with a better prognosis.
-
Extent of tumor residual. Resection is surgery to remove a tumor. Residual refers to how much of the tumor remains in the body after surgery. A patient’s prognosis is better when all of the tumor can be surgically removed. Whenever possible, surgery to remove all or most of the tumor should be considered if the surgical team and the patient feel the risk of such a surgery is acceptable. There are 4 classifications:
-
Gross total: The entire tumor that could be seen was removed. However, microscopic cells may remain.
-
Near total or subtotal: Large portions of the tumor were removed.
-
Partial: Only part of the tumor was removed.
-
Biopsy only: Only a small portion was removed and used for diagnostic tests.
-
-
Tumor location. A tumor can form in any part of the brain. Some tumor locations cause more damage than others, and some tumors are harder to treat because of their location.
-
Molecular features. Certain genetic mutations or changes to the genes found in the tumor may help determine prognosis. These include: IDH1 , IDH2 , MGMT , BRAF , H3K27M , and a 1p/19q codeletion. Sometimes, whether a tumor has any of these mutations or changes determines the type of brain tumor that is diagnosed.
-
Functional neurologic status. The doctor will test how well a patient is able to function and carry out everyday activities by using a functional assessment scale, such as the Karnofsky Performance Scale (KPS), outlined below. A higher score indicates a better functional status. Typically, someone who is better able to walk and care for themselves has a better prognosis.
-
100: Normal, no complaints, no evidence of disease
-
90: Able to carry on normal activity; minor symptoms of disease
-
80: Normal activity with effort; some symptoms of disease
-
70: Cares for self; unable to carry on normal activity or active work
-
60: Requires occasional assistance but is able to care for needs
-
50: Requires considerable assistance and frequent medical care
-
40: Disabled, requires special care and assistance
-
30: Severely disabled; hospitalization is indicated, but death not imminent
-
20: Very sick, hospitalization necessary; active treatment necessary
-
10: Approaching death, fatal processes progressing rapidly
-
-
Metastatic spread. A tumor that starts in the brain or spinal cord, even if cancerous, rarely spreads to other parts of the body in adults, but it may grow within the CNS. For that reason, with few exceptions, tests looking at the other organs of the body are typically not needed. A tumor that does spread to other parts of the brain or spinal cord is linked with a poorer prognosis.
-
Recurrent tumor. A recurrent tumor is one that has come back after treatment. If the tumor does return, there will be another round of tests to learn about the extent of the recurrence. These tests and scans are often similar to those done at the time of the original diagnosis.
Currently, the factors listed above are the best indicators of a patient’s prognosis. As discussed in Diagnosis , researchers are currently looking for biomarkers in the tumor tissue that could make a brain tumor easier to diagnose and allow for the staging of an adult brain tumor in the future. Researchers are also looking at other genetic tests that may predict a patient’s prognosis. These tools may someday help doctors predict the chance that a brain tumor will grow, develop more effective treatments, and more accurately predict prognosis.
Used with permission of the American College of Surgeons, Chicago, Illinois. The original and primary source for this information is the AJCC Cancer Staging Manual, Eighth Edition (2017), published by Springer International Publishing.
Information about the tumor’s grade, as well as the prognostic factors, will help the doctor recommend a specific treatment plan. The next section in this guide is Types of Treatment . Use the menu to choose a different section to read in this guide.
Brain Tumor - Types of Treatment
ON THIS PAGE: You will learn about the different types of treatments doctors use for people with a brain tumor. Use the menu to see other pages.
This section explains the types of treatments, also known as therapies, that are the standard of care for a brain tumor. “Standard of care” means the best treatments known. Information in this section is based on medical standards of care for a brain tumor in the United States. Treatment options can vary from one place to another.
When making treatment plan decisions, you are encouraged to discuss with your doctor whether clinical trials offer additional options to consider. A clinical trial is a research study that tests a new approach to treatment. Doctors learn through clinical trials whether a new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option for all types of brain tumors. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
How a brain tumor is treated
In brain tumor care, different types of doctors who specialize in cancer, called oncologists, often work together to create a patient’s overall treatment plan that combines different types of treatment. This is called a multidisciplinary team. Your care team may include other health care professionals, such as physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, dietitians, physical therapists, occupational therapists, rehabilitation specialists, and others. It is important to have a care team that specializes in caring for people with a brain tumor, which may mean talking with medical professionals beyond your local area to help with diagnosis and treatment planning. Learn more about the clinicians who provide cancer care.
Treatment options and recommendations depend on several factors:
-
The size, type, and grade of the tumor
-
Whether the tumor is putting pressure on vital parts of the brain
-
If the tumor has spread to other parts of the central nervous system (CNS) or body
-
Possible side effects
-
The patient’s preferences and overall health
Some types of brain tumors grow rapidly; other tumors grow slowly. Considering all these factors, your doctor will talk with you about how soon treatment should start after diagnosis.
For a low-grade brain tumor, surgery may be the only treatment needed, especially if all of the tumor can be removed in younger patients. If there is visible tumor remaining after surgery, radiation therapy and chemotherapy may be used. For higher-grade tumors, treatment usually begins with surgery, followed by radiation therapy and chemotherapy, often after a period of recovery. Your exact treatment plan will be developed with your health care team.
Successfully treating brain tumors can be challenging. The body’s blood-brain barrier normally protects the brain and spinal cord from harmful chemicals. This barrier also keeps out many types of chemotherapy. Surgery can be difficult if the tumor is near a delicate part of the brain or spinal cord. Even when the surgeon can completely remove the original tumor, parts of the tumor may remain that are too small to be seen or removed during surgery. Radiation therapy can also damage healthy tissue.
However, research in the past 20 years has helped to significantly lengthen the lives and improved the quality of life for many people with a brain tumor. These advancements include more refined surgeries, a better understanding of which types of tumors respond to chemotherapy and other drugs, and more targeted delivery of radiation therapy.
Take time to learn about all of your treatment options and be sure to ask questions about things that are unclear. Talk with your doctor about the goals of each treatment and what you can expect while receiving the treatment. These types of conversations are called “shared decision-making.” Shared decision-making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision-making is important for a brain tumor because there are different treatment options. Learn more about making treatment decisions .
Treatment options include those described below, such as surgery, radiation therapy, chemotherapy, and targeted therapy. Your care plan may also include treatment for symptoms and side effects, an important part of your medical care.
-
Physical, emotional, social, and financial effects of a brain tumor
-
Surgery
-
Radiation therapy
-
Chemotherapy
-
Targeted therapy
-
Alternating electric field therapy (tumor treating fields)
-
Treatment options by brain tumor type
-
Remission and the chance of recurrence
-
Metastatic cancer
-
If treatment does not work
Physical, emotional, social, and financial effects of a brain tumor
A brain tumor and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative and supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the tumor.
Palliative and supportive care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of tumor, may receive this type of care. And it often works best when it is started right after a brain tumor diagnosis. People who receive palliative and supportive care along with treatment for the tumor often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments, such as chemotherapy, surgery, or radiation therapy, to improve symptoms.
Some of the symptoms of a brain tumor can be severe and have an enormous impact on the daily lives of patients and their family caregivers. However, many symptoms can often be managed with the use of certain medications. Supportive care for people with a brain tumor includes:
-
Corticosteroids. These drugs are used to lower swelling in the brain, which can lessen headache pain from the swelling without the need for prescription pain medications. These drugs may also help improve neurological symptoms by decreasing the pressure from the tumor and swelling in the healthy brain tissue.
-
Anti-seizure medicines. These help control seizures, and there are several types of drugs available. These medications are prescribed by your neurologist.
Before treatment begins, talk with your doctor about the goals of each treatment in the recommended treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative and supportive care options. Many patients also benefit from talking with a social worker and participating in support groups. Ask your doctor about these resources, too.
Treatment for a brain tumor is often expensive, and navigating health insurance can be difficult. Ask your doctor or another member of your health care team about talking with a financial navigator or counselor who may be able to help with your financial concerns .
During treatment, your health care team may ask you to answer questions about your symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative and supportive care in a separate section of this website.
Return to top
Surgery
Surgery is the removal of the tumor and some surrounding healthy tissue during an operation. It is usually the first treatment used for a brain tumor. It is often the only treatment needed for a low-grade brain tumor. Removing the tumor can improve neurological symptoms, provide tissue for diagnosis and genetic analysis, help make other brain tumor treatments more effective, and, in many instances, improve the prognosis of a person with a brain tumor.
A neurosurgeon is a doctor who specializes in surgery on the brain and spinal column. Surgery to the brain requires the removal of part of the skull, a procedure called a craniotomy. After the surgeon removes the tumor, the patient's own bone will be used to cover the opening in the skull.
There have been rapid advances in surgery for brain tumors, including the use of cortical mapping, enhanced imaging, and fluorescent dyes.
-
Cortical mapping allows doctors to identify areas of the brain that control the senses, language, and motor skills.
-
Enhanced imaging devices give surgeons more tools to plan and perform surgery. For example, computer-based techniques, such as image guided surgery (IGS), help surgeons map out the location of the tumor very accurately. However, this is a very specialized technique that may not be widely available.
-
A fluorescent dye, called 5-aminolevulinic acid, can be given by mouth the morning before surgery. This dye is taken up by tumor cells. Doctors can use a special microscope and light to see the cells that have taken up the dye during the surgery. This helps doctors safely remove as much of the tumor as possible.
For a tumor that is near the brain’s speech center, it is increasingly common to perform the operation when the patient is awake for part of the surgery. Typically, the patient is awakened once the surface of the brain is exposed. Then, special electrical stimulation techniques are used to locate the specific part of the brain that controls speech. This approach can help avoid causing damage while removing the tumor.
In addition to removing or reducing the size of the brain tumor, surgery can provide a tissue sample for an analysis using a biopsy (see Diagnosis ). For some tumor types, the results of the biopsy can help determine if cancer medications or radiation therapy will be useful. For a cancerous tumor, even if it cannot be cured, removing it can relieve symptoms from the tumor pressing on the brain.
Sometimes, surgery cannot be performed because the tumor is located in a place the surgeon cannot reach or it is near a vital structure. These tumors are called inoperable or unresectable. If the tumor is inoperable, the doctor will recommend other treatment options that may also include a biopsy or removal of a portion of the tumor.
-
Laser interstitial thermal therapy (LITT) is a newer technique that can sometimes be used to treat malignant brain tumors that are unresectable. Following a biopsy to confirm the presence of the tumor, the neurosurgeon inserts a catheter containing a rotating laser, which can be used to heat up and eliminate the zone of tumor surrounding the catheter tip. This procedure is performed with the help of an intraoperative magnetic resonance imaging (MRI) scan that produces real-time images of the volume of tissue that is being heated. This is done to allow the neurosurgeon to carefully control and limit the effects of the LITT to the surrounding tumor and avoid damaging healthy brain tissue.
Before surgery, talk with your health care team about the possible side effects from the specific surgery you will have. Learn more about the basics of surgery .
Return to top
Radiation therapy
Radiation therapy is the use of high-energy x-rays or other particles to destroy tumor cells. Doctors may use radiation therapy to slow or stop the growth of a brain tumor. It is typically given after surgery and possibly along with chemotherapy. A doctor who specializes in giving radiation therapy to treat a tumor is called a radiation oncologist.
The most common type of radiation treatment is called external-beam radiation therapy, which is radiation given from a machine outside the body. When radiation treatment is given using implants, it is called internal radiation therapy or brachytherapy. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
External-beam radiation therapy can be directed at a brain tumor in the following ways:
-
Conventional radiation therapy. The treatment location is determined based on anatomic landmarks and x-rays. In certain situations, such as whole-brain radiation therapy for brain metastases, this technique is appropriate. For more precise targeting, different techniques are needed. The amount of radiation given depends on the tumor’s grade.
-
3-dimensional conformal radiation therapy (3D-CRT). Using images from computed tomography (CT) and magnetic resonance imaging (MRI) scans (see Diagnosis ), a 3-dimensional model of the tumor and healthy tissue surrounding the tumor is created on a computer. This model can be used to aim the radiation beams directly at the tumor, sparing the healthy tissue from high doses of radiation therapy.
-
Intensity modulated radiation therapy (IMRT). IMRT is a type of 3D-CRT (see above) that can more directly target a tumor. It can deliver higher doses of radiation to the tumor while giving less to the surrounding healthy tissue. In IMRT, the radiation beams are broken up into smaller beams and the intensity of each of these smaller beams can be changed. This means that the more intense beams, or the beams giving more radiation, can be directed only at the tumor.
-
Proton therapy. Proton therapy is a type of external-beam radiation therapy that uses protons rather than x-rays. At high energy, protons can destroy tumor cells. Proton beam therapy is typically used for tumors when less radiation is needed because of the location. This includes tumors that have grown into nearby bone, such as the base of skull, and those near the optic nerve.
-
Stereotactic radiosurgery. Stereotactic radiosurgery is the use of a single, high dose of radiation given directly to the tumor and not healthy tissue. It works best for a tumor that is only in 1 area of the brain and certain noncancerous tumors. It can also be used when a person has more than 1 metastatic brain tumor. There are many different types of stereotactic radiosurgery equipment, including:
-
A modified linear accelerator is a machine that creates high-energy radiation by using electricity to form a stream of fast-moving subatomic particles.
-
A Gamma Knife is another form of radiation therapy that concentrates highly focused beams of gamma radiation on the tumor.
-
A Cyber Knife is a robotic device used in radiation therapy to guide radiation to the tumor, particularly in the brain, head, and neck regions.
-
-
Fractionated stereotactic radiation therapy. Radiation therapy is delivered with stereotactic precision but divided into small daily doses called fractions and given over several days or weeks, in contrast to the 1-day radiosurgery. This technique is used for tumors located close to sensitive structures, such as the optic nerves or brain stem.
With these different techniques, doctors are trying to be more precise and reduce radiation exposure to the surrounding healthy brain tissue. Depending on the size and location of the tumor, the radiation oncologist may choose any of the above radiation techniques. In certain situations, a combination of multiple techniques may work best.
Short-term side effects from radiation therapy may include fatigue, mild skin reactions, hair loss, upset stomach, and neurologic symptoms, such as memory problems. Most side effects go away soon after treatment is finished. Also, radiation therapy is usually not recommended for children younger than 5 because of the high risk of damage to their developing brains. Longer term side effects of radiation therapy depend on how much healthy tissue received radiation and include memory and hormonal problems and cognitive (thought process) changes, such as difficulty understanding and performing complex tasks.
Learn more about the basics of radiation therapy .
Return to top
Therapies using medication
The treatment plan may include medications to destroy tumor cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy. Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body.
This treatment is generally prescribed by a neuro-oncologist, who is either a medical oncologist or neurologist physician who specializes in treating brain cancer with medication.
Medications are often given through an intravenous (IV) tube placed into a vein using a needle or as a pill or capsule that is swallowed (orally). It may also be given through a catheter or port , which are used to make IV injections easier. If you are given oral medications to take at home, be sure to ask your health care team about how to safely store and handle them.
The types of medications used for a brain tumor include:
-
Chemotherapy
-
Targeted therapy
Each of these types of therapies is discussed below in more detail. A person may receive 1 type of medication at a time or a combination of medications given at the same time. They can also be given as part of a treatment plan that includes surgery and/or radiation therapy.
The medications used to treat a brain tumor are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications.
It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with the medications used for a brain tumor, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases .
Chemotherapy ( updated 10/2023 )
Chemotherapy is the use of drugs to destroy tumor cells, usually by keeping the tumor cells from growing, dividing, and making more cells.
A chemotherapy regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A patient may receive 1 drug at a time or a combination of different drugs given at the same time. The goal of chemotherapy can be to destroy tumor cells remaining after surgery, slow a tumor’s growth, or reduce symptoms.
As explained above, chemotherapy to treat a brain tumor is typically given after surgery and possibly with or after radiation therapy, particularly if the tumor has come back after initial treatment.
Some drugs are better at going through the blood-brain barrier. These are the drugs often used for a brain tumor, such as temozolomide (Temodar), lomustine (CCNU), or others.
-
For people with glioblastoma and high-grade glioma, the latest standard of care is radiation therapy with daily low-dose temozolomide. This is followed by monthly doses of temozolomide after radiation therapy for 6 months to 1 year.
-
For people with anaplastic astrocytoma that is newly diagnosed or has not responded to treatment, temozolomide may be part of the recommended treatment plan.
-
A combination of 3 drugs, lomustine, procarbazine (Matulane), and vincristine (Vincasar), has been used along with radiation therapy. This combination is sometimes called PCV. This approach has helped lengthen the lives of patients with grade 2 or 3 oligodendroglioma with a 1p/19q codeletion (see also, "Molecular features" in the Grades and Prognostic Factors section) when given either before or, more commonly, right after radiation therapy. It has also been shown to lengthen lives of patients after radiation therapy for a low-grade glioma that could not be completely removed with surgery, particularly those low-grade tumors which have mutations of the IDH gene. Clinical trials on the use of chemotherapy to delay radiation therapy for patients with low-grade glioma are ongoing, as are clinical trials to determine if temozolomide can be substituted for PCV in the patients described above.
-
Gliadel wafers are a way to give the drug carmustine (BiCNU). These wafers are placed in the area where the tumor was removed during surgery.
Patients are monitored with brain magnetic resonance imaging (MRI) every 2 to 3 months while receiving active treatment. Then, the length of time between MRI scans increases depending on the tumor’s grade. Patients often have regular MRIs to monitor their health after treatment is finished and the tumor has not grown. If the tumor grows during treatment, other treatment options will be considered.
The side effects of chemotherapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, hair loss, loss of appetite, and diarrhea. These side effects usually go away after treatment is finished. Rarely, certain drugs may cause some hearing loss. Others may cause kidney damage. Patients may be given extra fluid by IV to protect their kidneys.
Learn more about the basics of chemotherapy .
Return to top
Targeted therapy
In addition to standard chemotherapy, targeted therapy is another way doctors use medication to treat cancer. Targeted therapy is a treatment that targets the tumor’s specific genes, proteins, or the tissue environment that contributes to a tumor’s growth and survival. This type of treatment blocks the growth and spread of tumor cells and limits the damage to healthy cells.
Not all tumors have the same targets, and some tumors may have more than 1 target. To find the most effective treatment, your doctor may run tests to identify the genes, proteins, and other factors in your tumor. This is called biomarker or molecular testing. This helps doctors better match each patient with the most effective treatment whenever possible. In addition, research studies continue to find out more about specific molecular targets and new treatments directed at them. Learn more about the basics of targeted treatments .
For a brain tumor, there are several types of targeted therapy that may be used:
-
Bevacizumab (Avastin, Mvasi) is an anti-angiogenesis therapy used to treat glioblastoma multiforme when previous treatment has not worked. Anti-angiogenesis therapy is focused on stopping angiogenesis, which is the process of making new blood vessels. Because a tumor needs the nutrients delivered by blood vessels to grow and spread, the goal of anti-angiogenesis therapy is to “starve” the tumor. ASCO does not recommend bevacizumab for people with newly diagnosed grade 4 glioblastoma that does not have an IDH mutation.
-
Larotrectinib (Vitrakvi) and entrectinib (Rozlytrek) are a type of targeted therapy that is not specific to a certain type of tumor but focuses on a specific genetic change called an NTRK fusion. This type of genetic change is found in a range of tumors, including some brain tumors. These drugs are approved to treat some brain tumors that are metastatic or cannot be removed with surgery and have worsened with other treatments.
-
Dabrafenib (Tafinlar) with trametinib (Mekinist) are approved for use in combination in tumors that contain BRAF mutations. These drugs can be effective in adult and pediatric malignant brain tumors, including gliomas, that contain BRAF mutations, particularly the V600E BRAF mutation.
A variety of other targeted therapies are being studied in brain tumors that contain other specific molecular changes, such as IDH and FGFR fusions. Talk with your doctor about the possible side effects for a specific medication and how they can be managed.
Return to top
Alternating electric field therapy (tumor treating fields)
This type of treatment uses a noninvasive portable device that interferes with the parts of a cell that are needed for tumor cells to grow and spread. It is given by placing electrodes that produce an electric field on the outside of a person’s head. The available device is called Optune.
Alternating electrical field therapy may be an option for people newly diagnosed with glioblastoma or for those with recurrent glioblastoma. Researchers have found that people with recurrent glioblastoma who used the device lived as long as those who received chemotherapy. In addition, they had fewer side effects. Other research shows that people newly diagnosed with glioblastoma lived longer and were less likely to have the disease worsen when this treatment was used along with temozolomide after radiation therapy. This treatment approach is now considered a recommended option for people with glioblastoma.
Return to top
Treatment options by brain tumor type
-
Oligodendroglioma. For people with grade 2 or grade 3 oligodendroglioma with a 1p/19q codeletion and an IDH genetic mutation (see Diagnosis ), ASCO recommends radiation therapy in combination with the chemotherapy drugs lomustine, procarbazine, and vincristine, which together are called PCV (see “Chemotherapy,” above). When radiation therapy and chemotherapy are given at the same time, it is called chemoradiation. For certain people with this type of grade 2 tumor, treatment may not begin until the tumor causes symptoms or imaging scans show that the tumor is growing.
-
Astrocytoma. ASCO recommends that people with grade 2 astrocytoma with an IDH genetic mutation and no 1p/19q codeletion be offered radiation therapy followed by chemotherapy with either the single drug temozolomide (Temodar) or with the PCV combination. Some people with this type of grade 2 tumor may be able to delay treatment until the tumor causes symptoms or imaging scans show that the tumor is growing. People with grade 3 astrocytoma with an IDH genetic mutation and no 1p/19q codeletion should be offered radiation therapy followed by temozolomide or both of these treatments given at the same time. Likewise, people with grade 4 astrocytoma with an IDH genetic mutation may be offered radiation therapy followed by temozolomide or both of these treatments given at the same time. Some astrocytomas without an IDH mutation may be treated the same way as glioblastoma that also does not have an IDH mutation (see below).
-
Glioblastoma. For most people with newly diagnosed grade 4 glioblastoma or a grade 2 or 3 astrocytoma and no IDH genetic mutation, ASCO recommends treatment with radiation therapy and temozolomide chemotherapy given at the same time. After this treatment, 6 months of temozolomide is recommended. Alternating electric field therapy (see above) may also be recommended for grade 4 glioblastoma located in the upper part of the brain. If the recommended treatment regimen becomes too difficult to complete, the doctor will recommend treatment with supportive care, hypofractionated radiation therapy, and/or temozolomide.
This information is based on the ASCO and Society for Neuro-Oncology (SNO) guideline, “ Therapy for Diffuse Astrocytic and Oligodendroglial Tumors in Adults .” Please note that this link takes you to another ASCO website.
Return to top
Remission and the chance of recurrence
A remission is when the tumor cannot be detected in the body. A remission can be temporary or permanent.
For most primary brain tumors, despite imaging tests showing that the tumor growth is controlled or there are no visible signs of a tumor, it is common for a brain tumor to recur.
Patients will often continue to receive regular MRI scans to watch for a recurrence. This uncertainty causes many people to worry that the tumor will come back. It is important to talk with your doctor about the possibility of the tumor returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the tumor does return. Learn more about coping with the fear of recurrence .
If the tumor returns after the original treatment, it is called a recurrent tumor. A recurrent brain tumor generally comes back near where it originally started. Rarely, it may come back in another place or in several areas, which is called a multifocal recurrence.
If a recurrence happens, a new cycle of testing will begin to learn as much as possible about it. After this testing is done, you and your doctor will talk about the treatment options. Often the treatment plan will include the treatments described above such as surgery, radiation therapy, chemotherapy, and targeted therapy, but they may be used in a different combination or given at a different pace. Options may include:
-
Temozolomide
-
Bevacizumab
-
Alternating electric field therapy for people with recurrent high-grade glioma
-
Clinical trials studying new treatments
There is no single approach to treating a recurrent brain tumor, and your treatment plan will be based on many factors. Whichever treatment plan you choose, palliative and supportive care will be important for relieving symptoms and side effects. Your doctor may suggest clinical trials of new drugs that are being created and tested to treat brain tumors that may help with recurrent tumors. Many of these new drugs are called "molecular targeted therapies" because they are small in size, which means they can be taken by mouth and/or can target specific parts of the brain tumor cells (see "Targeted therapy," above). These new drugs are being tested either alone or in combination with standard chemotherapy. Learn more about clinical trials on brain tumor treatment in the Latest Research section.
People with a recurrent brain tumor sometimes experience emotions such as disbelief or fear. You are encouraged to talk with your health care team about these feelings and ask about support services to help you cope. It may also be helpful to talk with other patients, including through a support group. Learn more about dealing with a recurrence .
Return to top
Metastatic cancer
If cancer spreads from where it started to another part of the body, doctors call it metastatic cancer. If this happens, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan. Clinical trials might also be an option. Learn more about getting a second opinion before starting treatment, so you are comfortable with your chosen treatment plan.
For many people, a diagnosis of metastatic cancer is very stressful and difficult. You and your family are encouraged to talk about how you feel with doctors, nurses, social workers, or other members of your health care team. It may also be helpful to talk with other patients, such as through a support group or other peer support program.
Your treatment plan may include a combination of surgery, radiation therapy, targeted therapy, and immunotherapy, which is a type of treatment designed to boost the body's natural defenses to fight the tumor. Learn more about immunotherapy below and in the Latest Research section of this guide.
Treatment of brain metastases
If cancer spreads to the brain from another part of the body, it is called a brain metastasis, metastatic cancer, or a secondary brain tumor. Brain metastases have traditionally been treated with surgery or radiation therapy. Chemotherapy is not often used because the blood-brain barrier keeps many drugs from reaching the brain. In the past, chemotherapy was mostly used only if radiation therapy did not work. However, other medications like targeted therapy and another type of medication approach called immunotherapy are options for certain people. Current options for treating brain metastases include:
-
Surgery. Surgery is generally only an option for patients who have 1 or 2 areas of metastatic cancer in the brain, especially when the tumors are large and causing symptoms. On occasion, patients with multiple areas of cancer in the brain who have a single large lesion causing symptoms will also be considered for surgery. Some patients with more than 2 lesions that are located close to each other may also be able to have multiple lesions removed with surgery. Radiation therapy is most often given afterward and sometimes before.
-
Radiation therapy. For most people with 1 to 4 tumors, high-dose radiation therapy given using stereotactic techniques (see "Radiation therapy," above) is preferred. Some people with 5 to 10 tumors may also be offered stereotactic radiosurgery. Stereotactic radiosurgery focuses the radiation only on the tumor in the brain, and this can also help lessen the side effects. The dose of radiation may be given in 1 treatment, called a single fraction, or across multiple treatments, called multifraction. Whole-brain radiation therapy is radiation therapy given to the entire brain, and it may be an option for some people. If whole-brain radiation therapy is given, your doctor may recommend techniques to avoid exposing the hippocampus to radiation, if possible, and giving a medication called memantine (Namenda), which can help with thinking problems.
-
Targeted therapy. Some types of targeted therapy can enter brain tumors and are able to target specific genetic changes in cancer that reaches the brain from metastatic disease that began elsewhere. These include:
-
Osimertinib (Tagrisso) or icotinib (Conmana) for metastatic non-small cell lung cancer (NSCLC) that has a genetic change on the EGFR gene (icotinib is being tested in clinical trials and has not been approved by the U.S. Food and Drug Administration for this purpose.)
-
Alectinib (Alecensa), brigatinib (Alunbrig), or ceritinib (Zykadia) for metastatic NSCLC with a genetic change on the ALK gene
-
Tucatinib (Tukysa), trastuzumab (Herceptin), and capecitabine (Xeloda) may be used for HER2-positive metastatic breast cancer
-
Dabrafenib (Tafinlar) with trametinib (Mekinist) may be used for metastatic melanoma
-
-
Immunotherapy. Some types of immunotherapy have shown promise in treating brain metastases from lung cancer and melanoma. These include ipilimumab (Yervoy), nivolumab (Opdivo), and pembrolizumab (Keytruda). Immunotherapy is another type of cancer therapy using medication. Learn more about immunotherapy in the Latest Research section of this guide.
Below is a general summary of when and how surgery and radiation therapy are used to treat brain metastases:
-
People with up to 4 brain metastases generally receive stereotactic radiosurgery. If the brain metastases are large or causing symptoms due to pressure on the brain and the person is in general good health, they often receive surgery followed by stereotactic radiosurgery.
-
Treatment for people in relatively good health and with more than 4 tumors that cannot be removed with surgery or more than 2 tumors that were removed surgically may include stereotactic radiosurgery or whole brain radiation therapy.
-
People who also have metastatic cancer in parts of the body other than the brain usually continue their treatment regimen if the disease outside the brain is not worsening. If the disease is worsening, the treatment plan may be changed based on the recommendations for that type of metastatic cancer.
The information in this section is based on a joint guideline from ASCO, the Society for Neuro-Oncology (SNO), and the American Society for Radiation Oncology (ASTRO), “ Treatment for Brain Metastases ,” and ASCO’s endorsement of the ASTRO guideline, “ Radiation Therapy for Brain Metastases .” Please note that these links take you to a different ASCO website.
Treatment of leptomeningeal metastases
If cancer spreads to the meninges or the cerebrospinal fluid (CSF), it is called leptomeningeal metastases. People with leptomeningeal metastases may receive chemotherapy given directly into the CSF of the brain. This may be done with a lumbar puncture and is called intrathecal chemotherapy. Or it may be given using a catheter with a reservoir, called an Ommaya reservoir. Radiation therapy may also be an option.
Managing the symptoms and side effects of brain metastases
The symptoms of brain metastases depend on where in the brain the cancer has spread, how much cancer is in the brain, and how quickly it spreads.
Relieving a person's symptoms and side effects is an important part of cancer care. Treatment for symptoms can continue even when active treatment to cure or slow down the cancer stops. Be sure to talk with the health care team about new symptoms or changes to existing symptoms.
ASCO recommends the following options to help relieve symptoms of brain metastases:
-
Dexamethasone (available as a generic drug), a type of drug called a corticosteroid, to lower swelling in the brain and help improve neurological symptoms caused by the tumor and swelling in the healthy brain tissue.
-
Anti-seizure medications are only recommended for people who are having seizures.
Learn about other options to help manage the symptoms of brain metastases .
Return to top
If treatment does not work
Recovery from a brain tumor is not always possible. If the tumor cannot be cured or controlled, the disease may be called advanced or terminal.
This diagnosis is stressful, and for some people, an advanced brain tumor is difficult to discuss. However, it is important to have open and honest conversations with your health care team to express your feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families and is there to help. Making sure a person is physically comfortable, free from pain, and emotionally supported is extremely important.
Planning for your future care and putting your wishes in writing is important, especially at this stage of disease. Then, your health care team and loved ones will know what you want, even if you are unable to make these decisions. Learn more about putting your health care wishes in writing.
People who have an advanced brain tumor and who are expected to live less than 6 months may want to consider hospice care. Hospice care is designed to provide the best possible quality of life for people who are near the end of life. You and your family are encouraged to talk with your doctor or a member of your palliative care team about hospice care options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment can make staying at home a workable option for many families. Learn more about advanced care planning .
After the death of a loved one, many people need support to help them cope with the loss. Learn more about grief and loss .
Return to top
The next section in this guide is About Clinical Trials . It offers more information about research studies that are focused on finding better ways to care for people with a brain tumor. Use the menu to choose a different section to read in this guide.
Brain Tumor - About Clinical Trials
ON THIS PAGE: You will learn more about clinical trials, which are the main way that new medical approaches are studied to see how well they work. Use the menu to see other pages.
What are clinical trials?
Doctors and scientists are always looking for better ways to care for people with a brain tumor. To make scientific advances, doctors create research studies involving volunteers, called clinical trials. Every drug that is now approved by the U.S. Food and Drug Administration (FDA) was tested in clinical trials.
Clinical trials are used for all types and grades of brain tumors. Many focus on new treatments to learn if a new treatment is safe, effective, and possibly better than the existing treatments. These types of studies evaluate new drugs, different combinations of treatments, new approaches to radiation therapy or surgery, and new methods of treatment.
People who participate in clinical trials can be some of the first to get a treatment before it is available to the public. However, there are some risks with a clinical trial, including possible side effects and the chance that the new treatment may not work. People are encouraged to talk with their health care team about the pros and cons of joining a specific study.
Some clinical trials study new ways to relieve symptoms and side effects during treatment. Others study ways to manage the late effects that may happen a long time after treatment. Talk with your doctor about clinical trials for symptoms and side effects.
Deciding to join a clinical trial
People decide to participate in clinical trials for many reasons. For some, a clinical trial is the best treatment option available. Because standard treatments are not perfect, patients are often willing to face the added uncertainty of a clinical trial in the hope of a better result. Others volunteer for clinical trials because they know that these studies are a way to contribute to the progress in treating a brain tumor. Even if they do not benefit directly from the clinical trial, their participation may benefit future people with a brain tumor.
Insurance coverage and the costs of clinical trials differ by location and by study. In some programs, some of the expenses from participating in the clinical trial are reimbursed. In others, they are not. It is important to talk with the research team and your insurance company first to learn if and how your treatment in a clinical trial will be covered. Learn more about health insurance coverage of clinical trials .
Sometimes people have concerns that, in a clinical trial, they may receive no treatment by being given a placebo or a “sugar pill.” When used, placebos are usually combined with standard treatment in most cancer clinical trials. Study participants will always be told when a placebo is used in a study. Find out more about placebos in cancer clinical trials.
Patient safety and informed consent
To join a clinical trial, people must participate in a process known as informed consent. During informed consent, the doctor should:
-
Describe all of the treatment options, so that the person understands how the new treatment differs from the standard treatment.
-
List all of the risks of the new treatment, which may or may not be different than the risks of standard treatment.
-
Explain what will be required of each person in order to participate in the clinical trial, including the number of doctor visits, tests, and the schedule of treatment.
-
Describe the purposes of the clinical trial and what researchers are trying to learn.
Clinical trials also have certain rules called “eligibility criteria” that help structure the research and keep patients safe. You and the research team will carefully review these criteria together. You will need to meet all of the eligibility criteria in order to participate in a clinical trial. Learn more about eligibility criteria in clinical trials.
People who participate in a clinical trial may stop participating at any time, for personal or medical reasons. This may include that the new treatment is not working or there are serious side effects. Clinical trials are also closely monitored by experts who watch for any problems with each study. It is important that people participating in a clinical trial talk with their doctor and researchers about who will be providing their treatment and care during the clinical trial, after the clinical trial ends, and/or if they choose to leave the clinical trial before it ends.
Finding a clinical trial
Research through clinical trials is ongoing for all tumor types. For specific topics being studied for brain tumors, learn more in the Latest Research section.
Cancer.Net more information about clinical trials in other areas of the website, including a complete section on clinical trials .
There are many resources and services to help you search for clinical trials for a brain tumor, including the following services. Please note that these links will take you to separate, independent websites:
-
ClinicalTrials.gov. This U.S. government database lists publicly and privately supported clinical trials.
-
World Health Organization (WHO) International Clinical Trials Registry Platform. The WHO coordinates health matters within the United Nations. This search portal gathers clinical trial information from many countries’ registries.
Read more about the basics of clinical trials matching services .
In addition, you can find a free video-based educational program about clinical trials in another section of this website.
The next section in this guide is Latest Research . It explains areas of scientific research for brain tumors. Use the menu to choose a different section to read in this guide.
Brain Tumor - Latest Research
ON THIS PAGE: You will read about the scientific research being done to learn more about brain tumors and how to treat them. Use the menu to see other pages.
Doctors are working to learn more about brain tumors, ways to prevent them, how to best treat them, and how to provide the best care to people diagnosed with a brain tumor. The following areas of research may include new options for patients through clinical trials. Always talk with your doctor about the best diagnostic and treatment options for you.
-
Enhanced imaging tests. New techniques for imaging scans are being researched. These may help doctors better track how well treatment is working and watch for possible tumor recurrence or growth.
-
Biomarkers. Researchers are examining biomarker tests that may help diagnose a brain tumor, estimate a patient’s prognosis, and/or predict whether a specific treatment may work. As explained in Diagnosis , a biomarker is a substance found in your blood, urine, or body tissue. Biomarker tests give the doctor more information about the cancer.
-
Immunotherapy. Immunotherapy , also called biological response modifier (BRM) therapy, uses the body's natural defenses to fight cancer by improving your immune system’s ability to attack cancer cells. Different methods are being studied for brain tumors, such as the use of dendritic cells or the use of vaccines aimed against a specific molecule on the surface of the tumor cells. Several methods are currently being tested in clinical trials.
-
Oncolytic virus therapy. This therapy uses a virus that infects and destroys tumor cells, sparing healthy brain cells. It is currently being researched as a treatment for brain tumors.
-
Targeted therapy. As outlined in Types of Treatment , this type of medication therapy targets faulty genes or proteins in the tumor that contribute to a tumor’s growth and development. Research continues on the use of different therapies for brain tumors that target the different ways a tumor grows, how a tumor spreads, and how tumor cells can be destroyed.
-
Blood-brain barrier disruption. This technique temporarily disrupts the brain’s natural protective barrier to allow chemotherapy to more easily enter the brain from the bloodstream.
-
New drugs and combinations of drugs. Researchers are looking at using drugs currently available for other types of cancer as treatment for a brain tumor. In addition, combinations of drugs that target the different ways a tumor grows and spreads are being explored. Since tumors can develop resistance to chemotherapy, meaning the treatment stops working over time, another approach is to use a treatment that targets how tumor cells develop resistance.
-
Gene therapy. This type of therapy seeks to replace or repair abnormal genes that are causing or helping tumor growth.
-
Genetic research. Researchers are seeking more information about specific gene mutations and how they relate to the risk and growth of a brain tumor. In particular, The Cancer Genome Atlas Program is a large, ongoing effort by the U.S. National Institutes of Health to find out more about the link between genetics and glioma. Recent results include the discovery of 3 specific genetic mutations not previously linked to glioblastoma: NF1 , ERBB2 , and PIK3R1 . Other research is focused on how the MGMT gene and mutations of the IDH gene are linked to brain tumors. This information is useful to researchers and may eventually lead to advances in the diagnosis and treatment of glioma. Precision medicine approaches that target tumor-specific mutations are being explored.
-
Palliative and supportive care. Clinical trials are underway to find better ways of reducing symptoms and side effects of current brain tumor treatments to improve comfort and quality of life for patients.
Looking for More About the Latest Research?
If you would like more information about the latest areas of research in brain tumors, explore these related items that take you outside of this guide:
-
To find clinical trials specific to your diagnosis, talk with your doctor or search online clinical trial databases .
-
Visit the Cancer.Net Blog to review news and information about brain tumors, including recent research and news about treatment.
-
Listen to a podcast from an ASCO expert discussing highlights from the 2022 and 2021 ASCO Annual Meetings.
-
Get updates from Cancer.Net delivered right to your inbox. Subscribe to the Inside Cancer.Net email newsletter.
-
Visit the website of Conquer Cancer, the ASCO Foundation, to find out how to help support cancer research. Please note that this link takes you to a different ASCO website.
The next section in this guide is Coping with Treatment . It offers some guidance on how to cope with the physical, emotional, social, and financial changes that a brain tumor and its treatment can bring. Use the menu to choose a different section to read in this guide.
Brain Tumor - Coping with Treatment
ON THIS PAGE: You will learn more about coping with the physical, emotional, social, and financial effects of a brain tumor and its treatment. Use the menu to see other pages.
Every treatment for a brain tumor can cause side effects or changes to your body and how you feel. For many reasons, people do not experience the same side effects even when they are given the same treatment for the same type of tumor. This can make it hard to predict how you will feel during treatment.
READ MORE BELOW:
-
Coping with physical side effects
-
Coping with emotional and social effects
-
Coping with the costs of cancer care
-
Coping with barriers to care
-
Talking with your health care team about side effects
-
Caring for a loved one with a brain tumor
As you prepare to start treatment, it is normal to fear treatment-related side effects. It may help to know that your health care team will work to prevent and relieve side effects. This part of treatment is called palliative and supportive care. It is an important part of your treatment plan, regardless of your age or the stage of disease.
Coping with physical side effects
Common physical side effects from each treatment option for a brain tumor are described in the Types of Treatment section. Learn more about side effects of a brain tumor and its treatment, along with ways to prevent or control them . Changes to your physical health depend on several factors, including the tumor’s location and grade, the length and dose of treatment, and your general health.
Talk with your health care team regularly about how you are feeling. It is important to let them know about any new side effects or changes in existing side effects. If they know how you are feeling, they can find ways to relieve or manage your side effects to help you feel more comfortable and potentially keep any side effects from worsening.
You may find it helpful to keep track of your side effects so it is easier to talk about any changes with your health care team. Learn more about why tracking side effects is helpful .
Sometimes, side effects can last after treatment ends. Doctors call these long-term side effects. Side effects that occur months or years after treatment are called late effects . Treating long-term side effects and late effects is an important part of survivorship care. Learn more by reading the Follow-up Care section of this guide or talking with your doctor.
Return to top
Coping with emotional and social effects
You can have emotional and social effects after a brain tumor diagnosis. This may include dealing with a variety of emotions, such as sadness, anxiety, fear, or anger, or managing stress. Sometimes, people find it difficult to express how they feel to their loved ones. Some have found that talking to an oncology social worker, counselor, or member of the clergy can help them develop more effective ways of coping and talking about a brain tumor.
Patients and their families are encouraged to share their feelings with a member of their health care team. You can also find coping strategies for emotional and social effects in a separate section of this website. This section includes many resources for finding support and information to meet your needs.
Return to top
Coping with the costs of cancer care
Treatment for a brain tumor can be expensive. It may be a source of stress and anxiety for patients and their families. In addition to treatment costs, many people find they have extra, unplanned expenses related to their care. For some people, the high cost of medical care stops them from following or completing their treatment plan. This can put their health at risk and may lead to higher costs in the future. Patients and their families are encouraged to talk about financial concerns with a member of their health care team. Learn more about managing financial considerations in a separate part of this website.
Return to top
Coping with barriers to care
Some groups of people experience different rates of new cases of brain tumors and experience different outcomes from their medical diagnosis. These differences are called “health disparities.” Disparities are caused in part by real-world barriers to quality medical care and social determinants of health , such as where a person lives and whether they have access to food and health care. Disparities more often negatively affect racial and ethnic minorities , people with fewer financial resources , sexual and gender minorities (LGBTQ+) , adolescent and young adult populations , adults older than 65 , and people who live in rural areas or other underserved communities .
If you are having difficulty getting the care you need, talk with a member of your health care team or explore other resources that help support medically underserved people .
Return to top
Talking with your health care team about side effects
Before starting treatment, talk with your doctor about possible side effects. Ask:
-
Which side effects are most likely?
-
When are they likely to happen?
-
What can we do to prevent or relieve them?
-
When and who should I call about side effects?
Be sure to tell your health care team about any side effects that happen during treatment and afterward, too. Tell them even if you do not think the side effects are serious. This discussion should include physical, emotional, social, and financial effects.
Return to top
Caring for a loved one with a brain tumor
Family members and friends often play an important role in taking care of a person with a brain tumor. This is called being a caregiver. Caregivers can provide physical, practical, and emotional support to the patient, even if they live far away. Being a caregiver can also be stressful and emotionally challenging. One of the most important tasks for caregivers is caring for themselves .
Patients with a brain tumor often need a lot of support at home. Many patients may not be able to do activities important for their care, such as driving to and from appointments. And some may need modified living arrangements to accommodate physical challenges. This means that caregivers have a range of responsibilities on a daily or as-needed basis, including:
-
Providing support and encouragement
-
Talking with the health care team
-
Giving medications
-
Helping manage symptoms and side effects of the tumor and treatment
-
Coordinating medical appointments
-
Providing transportation
-
Assisting with meals
-
Helping with household chores
-
Handling insurance and billing issues
-
Anticipating changes in mood, personality, and thinking and knowing how to best cope with these changes
A caregiving plan can help caregivers stay organized and help identify opportunities to delegate tasks to others. It may be helpful to ask the health care team how much care will be needed at home and with daily tasks during and after treatment. Use this 1-page fact sheet to help make a caregiving action plan. This free fact sheet is available as a PDF, so it is easy to print.
Learn more about caregiving or read the ASCO Answers Guide to Caring for a Loved One With Cancer in English or Spanish .
Learn more about caring for a person with a brain tumor or metastatic brain cancer.
Return to top
Looking for More on How to Track Side Effects?
Cancer.Net offers several resources to help you keep track of your symptoms and side effects. Please note that these links will take you to other sections of Cancer.Net:
-
Cancer.Net Mobile: The free Cancer.Net mobile app allows you to securely record the time and severity of symptoms and side effects.
-
ASCO Answers Fact Sheets: Read 1-page fact sheets on anxiety and depression , constipation , diarrhea , and rash that provide a tracking sheet to record details about the side effect. These free fact sheets are available as a PDF, so they are easy to print, fill out, and give to your health care team.
Return to top
The next section in this guide is Follow-up Care. It explains the importance of checkups after treatment for a brain tumor is finished. Use the menu to choose a different section to read in this guide.
Brain Tumor - Follow-Up Care
ON THIS PAGE: You will read about your medical care after treatment for a brain tumor is completed and why this follow-up care is important. Use the menu to see other pages.
Care for people diagnosed with a brain tumor does not end when active treatment has finished. Your health care team will continue to check that the tumor has not come back, manage any side effects, and monitor your overall health. This is called follow-up care.
Your follow-up care may include regular physical examinations, medical tests, or both. Doctors want to keep track of your recovery in the months and years ahead. Many brain tumors are very likely to recur, or come back, so you should be routinely monitored for new symptoms and with regular magnetic resonance imaging (MRI) scans. How often you schedule follow-up visits and have scans depends on the type of the tumor and other factors, so your health care team will talk with you about your exact schedule. Cancer rehabilitation also may be recommended (see "Managing long-term and late side effects," below).
Learn more about the importance of follow-up care .
Watching for recurrence
One goal of follow-up care is to check for a recurrence, which means that the tumor has come back. A tumor recurs because small areas of tumor cells may remain undetected in the body or may survive the initial tumor treatment. Over time, these cells may increase in number until they show up on test results or cause signs or symptoms.
During follow-up care, a doctor familiar with your medical history can give you personalized information about your risk of recurrence. Your doctor will ask specific questions about your health. Some people may have blood tests or imaging tests done as part of regular follow-up care, but testing recommendations depend on several factors including the type and grade of tumor first diagnosed and the types of treatment given.
The anticipation before having a follow-up test or waiting for test results may add stress to you or a family member. This is sometimes called “scanxiety.” Learn more about how to cope with this type of stress .
Managing long-term and late side effects
Most people expect to have side effects when receiving treatment. However, it is often surprising to survivors that some side effects may linger beyond the treatment period. These are called long-term side effects. Other side effects called late effects may develop months or even years after treatment has ended. Long-term and late effects can include both physical and emotional changes.
Talk with your doctor about your risk of developing such side effects based on your diagnosis, your individual treatment plan, and your overall health. If you had a treatment known to cause specific late effects, you may have certain physical examinations, scans, or blood tests to help find and manage them.
As described in previous sections, a brain tumor and its treatment can affect how your brain functions and your overall well-being. For this reason, it is important for your health care team to evaluate your quality of life and your cognitive and functional abilities through specialized tests. These tests are typically given by a neuropsychologist. A neuropsychologist is a psychologist who has special training in the brain’s capacity and behaviors.
These evaluations could identify situations when specific rehabilitation treatments would be helpful. Options for rehabilitative therapy include:
-
Speech therapy
-
Occupational therapy
-
Counseling , such as with a social worker
-
Medications to reduce fatigue or enhance memory
-
Neuropsychological testing, which looks at the behavioral and mental changes caused by the tumor and its treatment
The goal of rehabilitation is to help people regain control over many aspects of their lives and remain as independent as possible. Learn more about rehabilitation .
Keeping personal health records
You and your doctor should work together to develop a personalized follow-up care plan. Be sure to discuss any concerns you have about your future physical or emotional health. The American Society of Clinical Oncology (ASCO) offers forms to help keep track of the treatment you received and develop a survivorship care plan when treatment is completed.
This is also a good time to talk with your doctor about who will lead your follow-up care. Some survivors continue to see their specialist, while others transition back to the care of their primary care doctor or another health care professional. This decision depends on several factors, including the type and grade of tumor, treatments received, side effects, health insurance rules, and your personal preferences.
If a doctor who was not directly involved in your care will lead your follow-up care, be sure to share your treatment summary and survivorship care plan forms with them and with all future health care providers. Details about your brain tumor treatment are very valuable to the health care professionals who will care for you throughout your lifetime.
The next section in this guide is Survivorship . It describes how to cope with challenges in everyday life after a brain tumor diagnosis. Use the menu to choose a different section to read in this guide.
Brain Tumor - Survivorship
ON THIS PAGE: You will read about how to cope with challenges in everyday life after a brain tumor diagnosis. Use the menu to see other pages.
What is survivorship?
The word “survivorship” is complicated because it means different things to different people. Common definitions include:
-
Having no signs of the tumor after finishing treatment.
-
Living with, through, and beyond the diagnosis. According to this definition, survivorship begins at diagnosis and continues during treatment and through the rest of a person’s life.
For some, the term “survivorship” itself does not feel right, and they may prefer to use different language to describe and define their experience. Sometimes long-term treatment will be used for months or years to manage or control a tumor. Living with a brain tumor indefinitely is not easy, and the health care team can help you manage the challenges that come with it . Everyone has to find their own path to name and navigate the changes and challenges that are the results of their diagnosis and treatment.
Survivors may experience a mixture of feelings, including joy, concern, relief, guilt, and fear. Some people say they appreciate life more after the diagnosis and have gained a greater acceptance of themselves. Others become very anxious about their health and uncertain about coping with everyday life. Feelings of fear and anxiety may still occur as time passes, but these emotions should not be a constant part of your daily life. If they persist, be sure to talk with a member of your health care team.
Survivors may feel some stress when their frequent visits to the health care team end after completing treatment. Often, relationships built with the health care team provide a sense of security during treatment, and people miss this source of support. This may be especially true when new worries and challenges surface over time, such as any late effects of treatment, emotional challenges including fear of recurrence, sexual health and fertility concerns, and financial and workplace issues.
Every survivor has individual concerns and challenges. With any challenge, a good first step is being able to recognize your fears and talk about them. Effective coping requires:
-
Understanding the challenge you are facing
-
Thinking through solutions
-
Asking for and allowing the support of others
-
Feeling comfortable with the course of action you choose
Whenever possible, participation in a support group with other people diagnosed with brain tumors is highly encouraged. This allows you to talk with people who have had similar first-hand experiences. Other options for finding support include talking with a friend or member of your health care team, individual counseling, or asking for assistance at the learning resource center of the place where you received treatment.
A new perspective on your health
For many people, survivorship serves as a strong motivator to make lifestyle changes.
People recovering from a brain tumor are encouraged to follow established guidelines for good health, such as not smoking, limiting alcohol, eating well, exercising regularly, and managing stress. Regular physical activity can help rebuild your strength and energy level. Your health care team can help you create an appropriate exercise plan based upon your needs, physical abilities, and fitness level. Learn more about making healthy lifestyle choices .
It is important to have recommended medical checkups and tests (see Follow-up Care ) to take care of your health.
Talk with your health care team to develop a survivorship care plan that is best for your needs.
Changing role of caregivers
Family members and friends may also go through periods of transition. A caregiver plays a very important role in supporting a person diagnosed with a brain tumor, providing physical, emotional, and practical care on a daily or as-needed basis. Many caregivers become focused on providing this support, especially if the treatment period lasts for many months or longer.
However, as treatment is completed, the caregiver's role often changes. Eventually, the need for caregiving related to the diagnosis will become much less or come to an end. Caregivers can learn more about adjusting to life after caregiving .
Looking for More Survivorship Resources?
For more information about survivorship, explore these related items. Please note that these links will take you to other sections of Cancer.Net:
-
ASCO Answers Guide to Cancer Survivorship: Get this 48-page booklet that helps people transition into life after treatment. It includes blank treatment summary and survivorship care plan forms. The free booklet is available as a PDF, so it is easy to print.
-
Survivorship Resources: Cancer.Net offers information and resources to help survivors cope, including specific sections for children , teens and young adults , and people over age 65 . There is also a main section on survivorship for people of all ages.
The next section offers Questions to Ask the Health Care Team to help start conversations with your medical care team. Use the menu to choose a different section to read in this guide.
Brain Tumor - Questions to Ask the Health Care Team
ON THIS PAGE: You will find some questions to ask your doctor or other members of the health care team, to help you better understand your diagnosis, treatment plan, and overall care. Use the menu to see other pages.
Talking often with the health care team is important to make informed decisions about your health care. These suggested questions are a starting point to help you learn more about your care and treatment. You are also encouraged to ask additional questions that are important to you. You may want to print this list and bring it to your next appointment, or download Cancer.Net’s free mobile app for a digital list and other interactive tools to manage your care. It may also be helpful to ask a family member or friend to come with you to appointments to help take notes.
Questions to ask after getting a diagnosis
-
What type of brain tumor do I have?
-
Where is the tumor located in my brain?
-
Is the tumor cancerous?
-
What is the tumor’s grade? What does this mean?
-
Can you explain my pathology report (laboratory test results) to me?
-
Will an experienced neuropathologist review my pathology slides?
-
Do you have reading material that would help me understand my disease?
-
Who will be leading my overall treatment?
-
Should I get a second opinion?
-
Do you attend expert meetings to discuss complicated tumor cases?
-
Are there brain tumor centers of excellence that you recommend I contact?
-
Does your practice include multidisciplinary care? What does this mean?
-
If I’m worried about managing the costs of medical care, who can help me?
-
Do you know of a local support group for people with brain tumors?
Questions to ask about choosing a treatment plan and managing side effects
-
What are my treatment options?
-
What types of research are being done for brain tumors in clinical trials? Do clinical trials offer additional treatment options for me?
-
How many brain tumors do you treat each year?
-
What treatment plan do you recommend? Why?
-
What is the goal of each treatment? Is it to eliminate the tumor, help me feel better, or both?
-
What are the possible side effects of each treatment, both in the short term and the long term?
-
Would any of these treatment options keep me from participating in a clinical trial in the future?
-
When should I start treatment?
-
Who will be part of my health care team, and what does each member do?
-
How will this treatment affect my daily life? Will I be able to work, exercise, and perform my usual activities?
-
Could this treatment affect my sex life? If so, how and for how long?
-
Could this treatment affect my ability to become pregnant or have children? If so, should I talk with a fertility specialist before treatment begins?
-
What level of caregiving will I need during treatment and recovery?
-
If I have questions or problems, who should I call?
Questions to ask about having surgery
-
What type of surgery will I have?
-
How long will the operation take?
-
How long will I be in the hospital?
-
Can you describe what my recovery from surgery will be like?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term effects of having this surgery?
Questions to ask about having radiation therapy
-
What type of treatment is recommended?
-
What is the goal of this treatment?
-
How long will it take to give this treatment?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about having therapies using medication
-
What type of treatment is recommended?
-
What is the goal of this treatment?
-
How long will it take to give this treatment?
-
Will I receive this treatment at a hospital or clinic? Or will I take it at home?
-
What side effects can I expect during treatment?
-
Who should I contact about any side effects I experience? And how soon?
-
What are the possible long-term or late effects of having this treatment?
-
What can be done to prevent or relieve the side effects?
Questions to ask about planning follow-up care
-
What is the chance that the tumor will come back? Should I watch for specific signs or symptoms?
-
What long-term side effects or late effects are possible based on the treatment I received?
-
After treatment, what follow-up tests will I need, and how often will those tests be needed?
-
How do I get a treatment summary and survivorship care plan to keep in my personal records?
-
When should I return to my primary care doctor for regular medical care?
-
Who will be leading my follow-up care?
-
What survivorship support services are available to me? To my family?
The next section in this guide is Additional Resources . It offers more resources on this website that may be helpful to you. Use the menu to choose a different section to read in this guide.
Brain Tumor - Additional Resources
ON THIS PAGE: You will find some helpful links to other areas of Cancer.Net that provide information about medical care and treatment. This is the final page of Cancer.Net’s Guide to Brain Tumors. Use the menu to go back and see other pages.
Cancer.Net includes many other sections about the medical and emotional aspects of a brain tumor for the person diagnosed and their family members and friends. This website is meant to be a resource for you and your loved ones from the time of diagnosis, through treatment, and beyond.
Here are a few links to help you explore other parts of Cancer.Net:
-
Read more about the first steps to take when you are diagnosed with a brain tumor .
-
Find out more about clinical trials as a treatment option.
-
Get information about managing the financial costs of medical care.
-
Learn more about coping with the emotions that a tumor can bring, including those within a family or a relationship.
-
Find a national, not-for-profit advocacy organization that may offer additional information, services, and support for people with a brain tumor.
-
Explore what to do when you finish active treatment .
-
Download Cancer.Net Mobile , a free app that includes a symptom and side effect tracker, medication reminders, and other interactive resources.
-
To find a range of information and insights from different voices on timely cancer topics, visit the Cancer.Net Blog .
-
Watch Cancer.Net videos with ASCO experts, patients, and caregivers explaining the basics of cancer treatment, side effects, survivorship, clinical trials, caregiving, and more.
This is the end of Cancer.Net’s Guide to Brain Tumors. Use the menu to choose a different section to read in this guide.